![]()
![]()
Xiangyang WuI; Cingting WangII; Xinyuan DuIII; Yongnan LiI; Fengxiao HeI; Qiming ZhaoI; Yong MaoI
DOI: 10.21470/1678-9741-2022-0417
ABSTRACT
Introduction: Ventricular septal rupture is an important high-mortality complication in the scope of myocardial infarctions. The effectiveness of different treatment modalities is still controversial. This meta-analysis compares the efficacy of percutaneous closure vs. surgical repair for the treatment of postinfarction ventricular septal rupture (PI-VSR).AMI = Acute myocardial infarction
CABG = Coronary artery bypass grafting
CI = Confidence interval
CNKI = China National Knowledge Infrastructure
CT = Conservative treatment
LV-RA = Left ventricular-right atrial
M-H = Mantel-Haenszel
MI = Myocardial infarction
NR = Not reported
OR = Odds ratio
PC = Percutaneous closure
PI-VSR = Postinfarction ventricular septal rupture
SR = Surgical repairct
INTRODUCTION
Myocardial infarction (MI) is an acute condition with high morbidity and mortality rates throughout the world. Postinfarction ventricular septal rupture (PI-VSR), which has an incidence of 1% to 2%, is a rare but clinically fatal postinfarction complication[1]. Conservative medicinal therapy alone is only appropriate for patients with hemodynamically inconsequential defects or those whose surgical risk is prohibitive due to the high death rate associated with untreated defects. This can be close to 80% at 30-day postinfarction[2].
Surgical repair is a common and established form of treatment, but it is extremely invasive and fraught with the possibility of residual shunts and recurrent perforation after the procedure. In patients with cardiogenic shock and respiratory failure, urgent PI-VSR surgical correction has been linked to a 40% death risk[3]. Patients with PI-VSR typically have a poor cardiac function and inadequate surgical trauma tolerance at the same time (especially those with poor physical fitness). With the advent of interventional techniques, percutaneous closure has become an additional therapy option for such patients. Although extracorporeal circulation difficulties, lengthy operations, and disturbance of the sternal structures are avoided with percutaneous closure, there is a chance that postoperative residual shunts and vascular issues will develop[4,5].
Most importantly, there is still conflicting data on the efficiency of these two treatment options. To investigate this comparison further, we conducted a meta-analysis of the pertinent literature to compare the clinical results of percutaneous vs. surgical repair for the treatment of PI-VSR.
METHODS
The components for this meta-analysis were reported using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (or PRISMA) statement, a 27-item checklist[6]. The research protocol has also been submitted to the International Platform of Registered Systematic Review and Meta-analysis Protocols (INPLASY2022100056).
Search Strategy
The following seven electronic databases were comprehensively searched: Wanfang Data, VIP, China National Knowledge Infrastructure (or CNKI), Web of Science, Cochrane Library, PubMed®, and Embase. There were no restrictions set on the language or date of the literature search. The searches began on September 30, 2022. Studies detailed the results for patients over the age of 18 years who underwent percutaneous closure surgery or surgical repair for PI-VSR. The search was developed based on the PICOS principals, and search terms were “ventricular septal rupture” OR “ventricular septal ruptures” OR “ventricular septal perforation” OR “septal rupture, ventricular” OR “septal ruptures, ventricular” AND “surgery” OR “percutaneous closure surgery”. We manually searched reference lists of retrieved publications (including reviews) to find studies that might be eligible.
Study Selection and Inclusion Criteria
All citations were exported into EndNote, and after removing duplicates, YM and XW evaluated the titles and abstracts considering the eligibility requirements (Table 1). To be included, only studies written in English were taken into consideration. For studies that, once reviewed, were found to be “included” or “uncertain”, full papers were obtained, and the publications were checked against the inclusion criteria again. Studies that had the most thorough data and had been consistently published were chosen for reporting. Any disputes over which studies should be chosen were settled through discussion, and a final decision was made by a third reviewer (CW).
| Inclusion criteria | Exclusion criteria | |
|---|---|---|
| Language | English | Non-English |
| Publication dates | All years | |
| Participants | Age ≥ 18 years old | Age < 18 years old |
| PI-VSR patients | Animal studies | |
| Not AMI-related ventricular septal rupture | ||
| Intervention | Surgical repair | Not according to the inclusion criteria |
| Percutaneous closure surgery | ||
| Study design | Randomized controlled trial | Case report |
| Case control study | Review | |
| Cohort study | Protocol | |
| Commentary | ||
| Letter | ||
| Outcome | In-hospital mortality | Data about mortality or another outcome not available |
| One-year mortality | ||
| Postoperative residual shunt | ||
| Cardiac function grade (class I or II) |
AMI=acute myocardial infarction; PI-VSR=postinfarction ventricular septal rupture

Data Extraction
Author, publication year, study design, interventions employed in the treatment or control groups, sample size, and meta-analysis results were all collected using a customized extraction form. The authors of these studies were not contacted for additional information.
Quality Assessment
Two reviewers evaluated the quality of all included research independently (YM and XW). The quality of any nonrandomized controlled trials was evaluated using the Newcastle-Ottawa Scale (or NOS)[7]. Every included study was evaluated using the “star system”. A total score of 5 or less was regarded as poor, a score of 6 or 7 as moderate, and a score of 8 or 9 as high. Discrepancies were resolved by consultation and agreement between the other two reviewers (XD and CW). The primary outcome was a comparison of in-hospital mortality between the two treatments. The secondary outcomes are comparison results of one-year mortality, postoperative residual shunts, and postoperative cardiac function.
Statistical Analysis
The Cochrane Collaboration’s Review Manager software version 5.3 was used for meta-analysis and Egger’s regression test. For dichotomous variables, the Mantel-Haenszel model was used to obtain odds ratio (OR) and 95% confidence interval (CI). Heterogeneity between studies was assessed by I2 statistics.
Values of 25, 50, and 75% were reported as low, moderate, and high degrees of heterogeneity, respectively. A subgroup analysis in the meta-analysis (focused on different study designs such as randomized controlled trials, prospective cohort studies, and retrospective studies) was conducted to lessen the heterogeneity. A P<0.05 was considered to be statistically significant. Egger’s regression model was used to detect publication bias when the number of studies analyzed was enough.
RESULTS
A summary of the study selection process is presented in Figure 1.
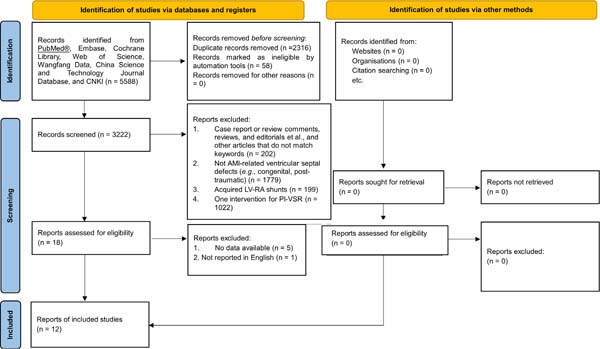

A total of 5,588 citations were found in the literature search. Of these, 2,374 research articles were eliminated for various reasons, including duplication. After reviewing the paper titles and abstracts, 3,024 articles were eliminated for PI-VSR or other reasons, depending on the type of article. Six papers were found to be invalid after the full-text versions of 18 publications were reviewed. Finally, 12 papers in total were down-selected and deemed suitable for analysis[8-19].
General Characteristics of the Included Studies
The key characteristics of the studies that fit the inclusion criteria are presented in Table 2. A total of 742 patients were included across these 12 papers, 459 of them fit the surgical repair group and 283 fit the percutaneous closure group. Six study groups within the papers analyzed compared surgical treatment with percutaneous closure. The other six groups of research evaluated surgical treatment, percutaneous closure, and conservative treatment. In terms of results, eleven of the studies looked at in-hospital mortality, three at one-year mortality, three at the residual shunt following surgery, and two at postoperative cardiac function.
| Study | Study type | Age, years | Male, n | Patients number | Intervention comparison | Time from AMI to operation, days | Defect size, mm | Outcomes | Occluder brand | Newcastle- Ottawa Scale scores |
|---|---|---|---|---|---|---|---|---|---|---|
| Rojas-Velasco et al., 2011 | Retrospective cohort study | 64 | 27 | 40 (15/7/18) | SR vs. PC vs. CT | 10.0 vs. 10.0 | NR | ①②④ | Amplatzer | 8 |
| Yinjun et al., 2013 | Retrospective cohort study | 68 | 2 | 11 (7/4) | SR vs. PC | NR | NR | ① | Shenzhen Lifetech (3) Amplatzer (1) | 7 |
| Kalyani et al., 2015 | Retrospective cohort study | 67 | 11 | 20 (14/6) | SR vs. PC | NR | NR | ① | Amplatzer | 8 |
| Goldsweig et al., 2017 | Retrospective cohort study | NR | 54 | 102 (91/11) | SR vs. PC | NR | NR | ② | NR | 7 |
| Yan et al., 2020 | Retrospective cohort study | 70.5 | 15 | 40 (3/16/11) | SR vs. PC vs. CT | NR | NR | ① | NR | 7 |
| Xuewen et al., 2020 | Retrospective cohort study | 66.5 | 37 | 66 (22/18/26) | SR vs. PC vs. CT | 31.6 vs. 20.4 | 13.0 vs. 13.0 | ①③ | Shanghai Shape Memory Alloy | 8 |
| Xinyu et al., 2020 | Retrospective cohort study | 62.6 | 21 | 31 (18/13) | SR vs. PC | NR | NR | ①② | NR | 7 |
| Bhattacharya et al., 2021 | Retrospective cohort study | 64.8 | 28 | 52 (22/5/25) | SR vs. PC vs. CT | NR | NR | ① | Amplatzer | 6 |
| Yaguo et al., 2021 | Retrospective cohort study | 71 | 18 | 50 (5/16/29) | SR vs. PC vs. CT | 14.0 vs. 19.0 | 10.6 vs. 13.1 | ① | NR | 7 |
| Dongliang et al., 2022 | Retrospective cohort study | 64.4 | 11 | 23 (17/6) | SR vs. PC | 35.1 vs. 29.3 | 10.0 vs. 10.0 | ①③④ | Shanghai Shape Memory Alloy | 9 |
| Giblett et al., 2022 | Retrospective cohort study | 68.8 | 289 | 362 (231/131) | SR vs. PC | 9.0 vs. 9.0 | 18.0 vs. 20.0 | ① | Amplatzer (127) Occlutech (4) | 8 |
| Zhenzhen et al., 2021 | Retrospective cohort study | 68.1 | 48 | 110 (14/50/46) | SR vs. PC vs. CT | NR | 24.3 vs. 11.9 | ①③ | NR | 8 |
① In-hospital mortality; ② one-year mortality; ③ postoperative residual shunt; ④ cardiac function AMI=acute myocardial infarction; CT=conservative treatment; NR=not reported; PC=percutaneous closure; SR=surgical repair

Primary Outcome
In-hospital Mortality
A statistically significant decrease was found when comparing in-hospital mortality in the surgical repair group to the percutaneous closure group (overall OR: 0.67, 95% CI 0.48-0.96, P=0.03) (Figure 2). Also, no heterogeneity was observed (I2=0%). The funnel plot is more symmetrical, suggesting less publication bias.
Secondary Outcomes
One-year Mortality
There were no significant differences observed in one-year mortality between the two therapy groups (overall OR: 0.58, 95% CI 0.24-1.39, P=0.23) (Figure 3). The groups showed only a moderate heterogeneity (I2=33%).
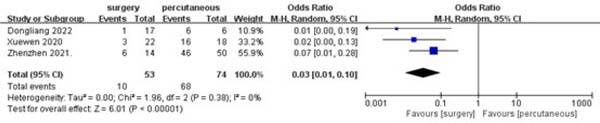
Postoperative Residual Shunt
A statistically significant decrease was found in the postoperative residual shunt frequency in the surgical repair group when compared to percutaneous closure (overall OR: 0.03, 95% CI 0.01-0.10, P<0.00001) (Figure 4). Also, no heterogeneity was observed (I2=0%).
Number of Postoperative Cardiac Function Grades (I or II)
A statistically significant increase was found in the number of postoperative cardiac function grades (I or II) in the surgical repair group when compared to percutaneous closure (overall OR: 3.89, 95% CI 1.10-13.74, P=0.04) (Figure 5). Also, high heterogeneity was observed in this group (I2=77%).


DISCUSSION
PI-VSR is an infrequent life-threatening complication following MI. This meta-analysis compared the effectiveness of percutaneous closure with that of surgical repair for PI-VSR. This investigation demonstrated that surgical repair had better postoperative cardiac function, lower incidence of a residual shunt, and lower in-hospital mortality than percutaneous closure. However, there was no statistically significant difference in one-year mortality between the two surgical strategies.
The dominant right coronary artery or the dominant left circumflex artery are the main causes of posterior septal perforation. This perforation occurs in the proximal 1/3 of the septum. An anterior septal rupture is in the distal 2/3 of the septum and is primarily caused by MI through the anterior wall due to occlusion of the left anterior descending artery. In addition to coronary revascularization, surgical methods were used to treat PI-VSR. Patients who also had concurrent ventricular aneurysms underwent ventriculotomy or ventriculoplasty[20]. Even though the technique is more invasive, the lesion is completely relieved. The patient’s postoperative recovery of heart function is consequently better facilitated by this surgical technique[21]. In addition, the following characteristics were linked to the occurrence of greater residual shunts in the percutaneous occlusion group than in the surgical repair group: (1) the perforated ventricular septum is typically irregular in shape, and the occluder chosen is too small to cause residual shunts or too large to cause complications like atrioventricular block and ventricular arrhythmias; (2) the tissue of the perforated ventricular septum after MI is brittle and there may be small gaps between the septum and the occluder after blocking, some of which may form after the blocking procedure; (3) the location of the defect following a severe inferior wall MI is frequently on the free wall at the base of the right and left ventricles, which has an impact on the occluder disc’s deployment[22-25].
The effectiveness of percutaneous intervention and surgical repair have not been previously compared in a meta-analysis. The effectiveness of this specific PI-VSR therapy modality has been carefully assessed by several researchers. Flynn[26] included 314 patients who underwent percutaneous occlusion of the PI-VSR in 25 trials, with an in-hospital mortality rate of 37.5%. Matteucci[27] included 6,361 patients in 41 studies with a surgical mortality rate of 38.2%. The surgical and percutaneous intervention groups each had an in-hospital death rate of 37.2% and 40.4%, totaling 742 patients, which was comparable to the outcomes of the two systems analyzed above. Furthermore, Ronco’s systematic[28] analysis found no statistically significant difference between contemporaneous coronary artery bypass grafting (CABG) and no CABG in the management of mechanical complications after MI in terms of immediate or long-term mortality. The magnitude of the PI-VSR defect was not related to death, according to Yang’s[29] study.
Limitations
This meta-analysis has several limitations. First, the included studies were all retrospective, and it was not possible to control potential confounding factors. Second, the use of various occluder brands could be an additional confounding factor. Finally, different intervention times could also be a confounding factor.
CONCLUSION
Acute MI complications like PI-VSR are uncommon, yet deadly. We conducted a meta-analysis and concluded that, for PI-VSR, surgery seems to be a safer therapeutic choice than percutaneous closure. In the future, large-scale randomized controlled trials are required to confirm the effects of percutaneous closure and surgical repair.
REFERENCES
1. Matteucci M, Ronco D, Corazzari C, Fina D, Jiritano F, Meani P, etal. Surgical repair of postinfarction ventricular septal rupture: systematicreview and meta-analysis. Ann Thorac Surg. 2021;112(1):326-37.doi:10.1016/j.athoracsur.2020.08.050. [MedLine]
2. Damluji AA, van Diepen S, Katz JN, Menon V, Tamis-Holland JE,Bakitas M, et al. Mechanical complications of acute myocardial infarction: ascientific statement from the American heart association. Circulation.2021;144(2):e16-e35. doi:10.1161/CIR.0000000000000985. [MedLine]
3. Deja MA, Szostek J, Widenka K, Szafron B, Spyt TJ, Hickey MS, et al.Post infarction ventricular septal defect - can we do better? Eur J CardiothoracSurg. 2000;18(2):194-201. doi:10.1016/s1010-7940(00)00482-6. [MedLine]
4. Shafiei I, Jannati F, Jannati M. Optimal time repair of ventricularseptal rupture post myocardial infarction. J Saudi Heart Assoc.2020;32(2):288-94. doi:10.37616/2212-5043.1120. [MedLine]
5. Jones BM, Kapadia SR, Smedira NG, Robich M, Tuzcu EM, Menon V, etal. Ventricular septal rupture complicating acute myocardial infarction: acontemporary review. Eur Heart J. 2014;35(31):2060-8.doi:10.1093/eurheartj/ehu248. [MedLine]
6. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj. n71.
7. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25(9):603-5. doi:10.1007/s10654-010-9491-z.
8. Rojas-Velasco G, Lerma C, Arias-Mendoza A, Álvarez-Sangabriel A, Altamirano A, Azar-Manzur F, et al. Características clínicas, modalidades de tratamiento y mortalidad en la ruptura del septum interventricular posinfarto. Arch Cardiol Mex. 2011;81(3):197-203.
9. Yinjun Zhao, Qiang Li, Zhanquan Li, et al. Treatment of acute myocardial infarction with ventricular septal perforation. Chin J Thorac Cardiovasc Surg. 2013;29(4):225-226.
10. Trivedi KR, Aldebert P, Riberi A, Mancini J, Levy G, Macia JC, et al. Sequential management of post-myocardial infarction ventricular septal defects. Arch Cardiovasc Dis. 2015;108(5):321-30. doi:10.1016/j. acvd.2015.01.005.
11. Goldsweig AM, Wang Y, Forrest JK, Cleman MW, Minges KE, Mangi AA, et al. Ventricular septal rupture complicating acute myocardial infarction: incidence, treatment, and outcomes among medicare beneficiaries 1999-2014. Catheter Cardiovasc Interv. 2018;92(6):1104- 15. doi:10.1002/ccd.27576.
12. Yan Shao, Nailiang Tian, Yi Shen, et al. Clinical characteristics and prognosis analysis of patients with acute myocardial infarction combined with ventricular septal perforation. Int J Cardiovasc Dis. 2020;47(5):311-314.
13. Xuewen Wang, Jianli Zhong, Hua Yan, et al. Clinical comparison of interventional occlusion and surgical treatment for acute myocardial infarction complicated with ventricular septal rupture. Chin J Intervent Cardiol. 2020;28(10):560-565.
14. Xinyu Tian, Pengcheng Li, Yanzhou Zhang, et al. Prognostic analysis of interventional therapy and surgical intervention for ventricular septal rupture. J Med Forum. 2020;41(5):37-43.
15. Bhattacharya D, Sambaturu VK, Harikrishnan KN, et al. Outcome of ventricular septal rupture from a tertiary care centre in South India. Indian Heart J. 2021;73:S52.
16. Yago Zheng,Dujiang Xie,Nailiang Tian,et al. Clinical analysis of 50 cases of acute myocardial infarction combined with ventricular septal perforation. J Nanj Med Univer (Natural Sciences). 2021;41(3):391-6.
17. Ma D, Zhang Z, Zhang S, Wang Z, Zhang G, Wang C, et al. Treatment strategies for ventricular septal rupture after myocardial infarction: a single-center experience. Front Cardiovasc Med. 2022;9:843625. doi:10.3389/fcvm.2022.843625.
18. Giblett JP, Matetic A, Jenkins D, Ng CY, Venuraju S, MacCarthy T, et al. Post-infarction ventricular septal defect: percutaneous or surgical management in the UK national registry. Eur Heart J. 2022;43(48):5020- 32. doi:10.1093/eurheartj/ehac511.
19. Zhenzhen Wang. Clinical analysis of different treatment methods for ventricular septal perforation after acute myocardial infarction . Zhengzhou University. 2021.
20. Shah AH, Puri R, Kalra A. Management of cardiogenic shock complicating acute myocardial infarction: a review. Clin Cardiol. 2019;42(4):484-93. doi:10.1002/clc.23168.
21. Topaz O. The enigma of optimal treatment for acute ventricular septal rupture. Am J Cardiol. 2003;92(4):419-20. doi:10.1016/s0002- 9149(03)00660-x.
22. Risseeuw F, Diebels I, Vandendriessche T, De Wolf D, Rodrigus IE. Percutaneous occlusion of post-myocardial infarction ventricular septum rupture. Neth Heart J. 2014;22(2):47-51. doi:10.1007/s12471- 013-0498-4.
23. Oman Z, Kumar S, Ghani A, Sayed-Ahmad Z, Horbal P, Nasir A, et al. Percutaneous repair of post-myocardial infarction ventricular septal rupture presenting with cardiogenic shock. Am J Cardiovasc Dis. 2020;10(4):376-81.
24. Baldasare MD, Polyakov M, Laub GW, Costic JT, McCormick DJ, Goldberg S. Percutaneous repair of post-myocardial infarction ventricular septal defect: current approaches and future perspectives. Tex Heart Inst J. 2014;41(6):613-9. Erratum in: Tex Heart Inst J. 2015;42(1):97. doi:10.14503/THIJ-13-3695.
25. Andersen MM, Zhao DXM. Percutaneous Post-Myocardial Infarction Ventricular Septal Rupture Closure: A Review. Struct Heart. 2018;2(2):121-6.
26. Flynn CD, Morris P, Manuel L, Matteucci M, Ronco D, Massimi G, et al. Systematic review and meta-analysis of the mechanical complications of ischemic heart disease: papillary muscle rupture, left ventricle rupture and post-infarct ventricular septal defect. Ann Cardiothorac Surg. 2022;11(3):195-209. doi:10.21037/acs-2022-ami-24.
27. Moreyra AE, Huang MS, Wilson AC, Deng Y, Cosgrove NM, Kostis JB, et al. Trends in incidence and mortality rates of ventricular septal rupture during acute myocardial infarction. Am J Cardiol. 2010;106(8):1095- 100. doi:10.1016/j.amjcard.2010.06.013.
28. Ronco D, Corazzari C, Matteucci M, Massimi G, Di Mauro M, Ravaux JM, et al. Effects of concomitant coronary artery bypass grafting on early and late mortality in the treatment of post-infarction mechanical complications: a systematic review and meta-analysis. Ann Cardiothorac Surg. 2022;11(3):210-25. doi:10.21037/acs-2021-ami-19.
29. Yang X, Yu Z, Wang Y, Ding Y, Ni R, Xiao P. Transcatheter closure for postinfarction ventricular septal defect: a meta-analysis of the current evidence. J Card Surg. 2021;36(12):4625-33. doi:10.1111/jocs.15989.
Authors’Roles & Responsibilities
XW= Substantial contributions to the conception and design of the work; and the analysis and interpretation of data for the work; drafting the article and revising it; final approval of the version to be published
CW= Substantial contributions to the acquisition, analysis, and interpretation of data for the work; revising the work critically for important intellectual content; final approval of the version to be published
XD= Substantial contributions to the acquisition, analysis, and interpretation of data for the work; revising the work critically for important intellectual content; final approval of the version to be published
YL= Substantial contributions to the analysis and interpretation of data for the work; revising the work critically for important intellectual content; final approval of the version to be publishe
FH= Substantial contributions to the acquisition and analysis of data for the work; revising the work critically for important intellectual content; final approval of the version to be published
QZ= Substantial contributions to the acquisition and analysis of data for the work; revising the work critically for important intellectual content; final approval of the version to be published
YM= Substantial contributions to the conception and design of the work; and the acquisition, analysis, and interpretation of data for the work; drafting the work and revising it; final approval of the version to be published
Article receive on Friday, November 11, 2022
Article accepted on Wednesday, November 23, 2022
 All scientific articles published at bjcvs.org are licensed under a Creative Commons license
All scientific articles published at bjcvs.org are licensed under a Creative Commons license













All rights reserved 2017 / © 2024 Brazilian Society of Cardiovascular Surgery
DEVELOPMENT BY ![]()





 English PDF
English PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket