ABSTRACT
OBJECTIVE: To assess the immediate result of the modified Norwood procedure with new technique of anterograde regional cerebral perfusion (ARCeP) and retrograde regional coronary perfusion (RRCoP) in substitution of profound hypothermia and circulatory arrest in children with hypoplastic left heart syndrome (HLHS) with extremely hypoplastic ascending aorta (HA). METHODS: In the period of December of 2006 to February 2008 the modified Norwood procedure with tube between the right ventricle and pulmonary arteries or Sano shunt was performed in eight children with HLHS and with ascending aorta diameter less than 3 mm, (four male and four female) with median age of 9.2 days (ranging from 1 to 29 days) and median weigh of 3.3 kg (ranging from 2.7 to 3.8 kg). We used cardiopulmonary bypass and hypothermia at 25ºC with two venous cannulas and suture with a polytetrafluoroethylene graft sutured to the innominate artery as an arterial line and used to ARCeP. The RRCoP was performed by a deviation in the arterial line and placement of a catheter in the ascending aorta. The immediate surgical results and the clinical neurological manifestation were assessed. RESULTS: The immediate surgical results revealed mortality of 25% and there were absence of neurological injury at clinical examination. CONCLUSIONS: The modified Norwood procedure can be accomplished with ARCeP and RRCoP in children with HLHS with HA with satisfactory immediate surgical result and without neurological complications.
RESUMO
OBJETIVO: Avaliar o resultado imediato da operação de Norwood modificado com nova técnica de perfusão regional cerebral (PRCeA) anterógrada associado a perfusão regional coronariana (PRCoR) retrógrada em substituição à parada circulatória total com hipotermia profunda em crianças portadoras da Síndrome da Hipoplasia do Coração Esquerdo (SHCE) com aorta ascendente extremamente hipoplásica (AH). MÉTODOS: No período de dezembro de 2006 a fevereiro de 2008, a operação de Norwood modificado com tubo entre o ventrículo direito e as artérias pulmonares ou shunt tipo Sano foi realizada em oito crianças portadoras de SHCE e aorta ascendente com diâmetro inferior a 3 mm, (quatro do sexo masculino e quatro do sexo feminino) com idade média de 9,2 dias (variando de 1 a 29 dias) e peso médio de 3,3 kg (variando de 2,7 a 3,8 kg). Utilizada CEC e hipotermia a 25ºC com duas cânulas venosas e anastomose de um enxerto de politetrafluoretileno com a artéria inominada utilizado como linha arterial e para PRCeA. A PRCoR foi realizada por meio de um desvio na linha arterial e colocação de um cateter na aorta ascendente. Foram analisados o resultado cirúrgico imediato e a presença de alterações neurológicas nesse período. RESULTADOS: O resultado cirúrgico imediato revelou mortalidade de 25% e ausência de comprometimento neurológico ao exame clínico. CONCLUSÃO: A operação de Norwood modificado pode ser realizada com PRCeA e PRCoR em crianças com SHCE e AH com resultado cirúrgico imediato satisfatório e ausência de complicações neurológicas.
INTRODUCTION
The Hypoplastic Left Heart Syndrome (HLHS) is a congenital heart defect presenting great morphological stenosis or atresia of the mitral valve and aortic valve stenosis or atresia associated with various degrees of hypoplastic left ventricle. The detailed study of anatomy is essential to propose the appropriate surgical treatment. The most common form of presentation of HLHS is the presence of mitral stenosis and aortic atresia, occurring in 36.1% of patients. The presence of aortic atresia in hypoplastic left heart syndrome is a substantial risk factor and is related to low cardiac output during the immediate postoperative period [1] and is often accompanied by extremely hypoplastic ascending aorta (AH) (smaller than 3 mm in diameter), influencing the performance of the right ventricle that would be more exposed to ischemia, as a result of the difficulty of aortic retrograde perfusion of the coronary arteries.
The neurological performance is an important concern in the treatment of HLHS and the use of cardiopulmonary bypass (CPB) associated with total circulatory arrest with deep hypothermia can help to increase the risk of neurological disorders. To reduce this risk factor, the use of CPB with regional anterograde cerebral perfusion (rACP) has been used to increase neuroprotection during aortic arch reconstruction and theoretically reduce the neurological damage [2]. The decrease in the aortic clamping (AC) may be an important factor in the preservation of right ventricular function, mainly when the ascending aorta has a diameter very hypoplastic. With the use of regional retrograde coronary perfusion (rRCorP) in this group of children it was possible to perform the Norwood procedure using a beating heart procedure, reducing the time of AC.
METHODS
From December 2006 to February 2008, we performed a modified Norwood operation with tube between the right ventricle and the pulmonary arteries or Sano's operation in eight children (four males and four females), mean age of 9.2 days (ranging from 1 to 29 days) and average weight of 3.3 kg (varying from 2.7 to 3.8 kg). The children had HLHS and AAH (Figure 1) with an average diameter of 2.3 mm (ranging from 2.0 to 3.0 mm). After completion of sternotomy, full-flow CPB was installed (100-150 ml/kg/ min) and hypothermia with nasopharyngeal temperature at 25°C with the administration of chlorpromazine (5 mg/kg) to reduce systemic vascular resistance. We used two venous cannulas and a 4 mm tube of polytetrafluoroethylene (PTFE) anastomosed in the innominate artery as arterial line and to perform rRCorP. The rRCorP was performed using a arterial line bypass (Figure 2) and placing a 4 or 6 French catheter in the ascending aorta (depending on the diameter of this vessel) at the junction between the ascending aorta and aortic arch (Figure 3).
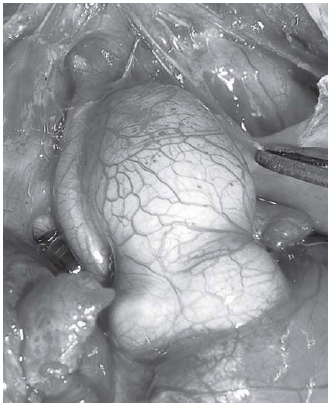
Fig. 1 - Extremely hypoplastic ascending aorta in children with hypoplastic left heart syndrome

Fig. 2 - Deviation in the arterial line to perform regional retrograde coronary perfusion

Fig. 3 - Catheter at the junction between the ascending aorta and aortic arch to perform regional retrograde coronary perfusion
To monitor the pressure during rACP it was used puncturing or dissection of the right radial artery. After the end of CPB, modified ultrafiltration was used.
With the heart beating it was performed right atriotomy and atrioseptectomy. The pulmonary trunk was sectioned near the origin of the right and left lung branches. The distal segment of the pulmonary trunk was closed with a fresh autologous pericardium patch, where a linear incision was performed to receive the distal anastomosis of the PTFE tube of the Sano's operation.
The diameter of the PTFE tube was 4 mm for children weighing less than 3.3 kg and 5 mm for children weighing more than 3.3 kilograms. After clamping of the descending aorta, clamping of the innominate artery proximal to the PTFE tube - with directioning of the flow to the brain circulation with a flow of 40 ml/kg/min to achieve a mean arterial pressure of 40 mmHg - and garroting of carotid and left subclavian arteries,it was performed section of the ascending aorta at the junction with the aortic arch, by maintaining the perfusion of coronary arteries with rRCorP.
After ligation and sectioning of the artery channel, the little curvature of the aortic arch was opened from the innominate artery to the descending aorta, the whole tissue of the ductus arteriosus was resected and the aorta was enlarged using fresh autologous pericardium and the neo-aorta was reconstructed performing the anastomosis of the PT with the aortic arch. At this point the surgery was performed with the heart beating as a result of the rRCorP. With administration of St. Thomas cardioplegia solution plus blood at a rate of 3/1 through the catheter used for the rRCorP, it was performed anastomosis of the ascending aorta with the neo-aorta (Figure 4). Finally, with the heart beating it was performed proximal anastomosis of the PTFE tube of Sano's operation on the right ventricle. All children were mantained with their sternum opened and subsequently underwent closure of the chest at the ICU. We analyzed in this group of children the mortality rate and the presence of neurological changes identified by routine physical examination.

Fig. 4 - Anastomosis of the hypoplastic ascending aorta with the neoaorta
The mean time of CPB was 145.7 minutes (ranging from 100 to 235 minutes) and mean time of aortic clamping was 29.7 minutes (ranging from 19 to 43 minutes). The surgical and hospital mortality was 25%. No child presented seizures or motor abnormalities identified on clinical examination.
DISCUSSION
Surgical repair of HLHS is a challenge. In the preoperative period it has great importance to preservation of the right ventricle, preventing ischemic events as a result of increased pulmonary flow and decreased systemic and coronary flow. The distribution of pulmonary and systemic flows is influenced by the size of the atrial septal defect, the type of ventilation and the type of vasoactive drugs used. There are several risk factors in children with HLHS and that may interfere with the surgical outcome. Jacobs et al. [3] identified a higher surgical risk in children with genetic syndromes, including Down syndrome and Turner syndrome and when there is heterotaxy, polysplenia, asplenia, biliary atresia and prematurity less than 35 weeks. Stasik et al. [4] identified the weight below 2.5 kg, gestational age, extracardiac abnormalities and genetic syndromes and risk factors. Gaynor et al. [5] identified as risk factors for operative mortality the birth weight and associated heart diseases and, in the one-year survival, the presence of extracardiac anomalies, cardiac defect and presence of genetic syndrome.
On the other hand, Wernovsky et al. [6] have not identified as increased risk factors the birth weight, genetic syndromes and length of surgery and noted as factors that increase morbidity: diaphragmatic paralysis, vocal cord injury, prolonged ventilation and seizures in the postoperative period. The use of an Aristotle risk score in the Norwood procedure showed a high correlation with mortality in the series presented by Sinzobahamvya et al. [7] in the presence of aortic atresia, interrupted aortic arch, preoperative mechanical ventilation, preoperative shock with a risk score greater than 20. These results were confirmed by Artrip et al. [8] in which the weight and an Aristotle risk score greater than 20 are accompanied by high mortality. In the study by McGuirk et al. [9] the authors showed that the body surface area, the ascending aortic diameter, right ventricular function and type of pulmonary blood flow were important risk factors for immediate mortality.
The size of the ascending aorta in hypoplastic left heart syndrome has implications for the choice of type of surgery to be adopted. The completion of the classical Norwood procedure when the ascending aorta has a very small diameter involves a long suture of a graft to the ascending aorta diminished, increasing the time of AC and myocardial damage, as confirmed by Delmo Walter et al. [10]. The presence of moderate or severe tricuspid valve insufficiency in HLHS is one of the factors that influence the outcome of the Norwood procedure. Ota et al. [11] has shown that the tricuspid regurgitation improved significantly after the Norwood procedure associated to Sano's operation due to the adequacy of pulmonary flow. The fulfillment of tricuspid valve repair also plays an important role in the preservation of right ventricular function [12,13].
The Norwood procedure is often performed using CPB associated with total circulatory arrest with deep hypothermia [14]. This procedure is not free of neurological complications and may increase the incidence of seizures during the immediate postoperative period and may cause delayed psychomotor development. The total circulatory arrest with deep hypothermia can also cause changes in coagulation factors, increasing morbidity during the immediate postoperative period. In order to avoid total circulatory arrest and deep hypothermia, Imoto et al. [15] performed the Norwood operation with CPB and moderate hypothermia using rACP through the anastomosis of a PTFE graft in the innominate artery and perfusion of the lower body segment by inserting an arterial cannula in the descending aorta (DAC), thus avoiding circulatory arrest and deep hypothermia, but not reducing the time of AC.
Tchervenkov et al. [16] performed the Norwood operation with rACP through retrograde perfusion of modified Blalock-Taussig shunt. This technique avoids total circulatory arrest, but using deep hypothermia and there is no concern about the decrease in the time of AC. Kishimoto et al. [17] performed the Norwood operation with the heart beating through rACP and DAC. In this technique variation, the pulmonary trunk is sutured to the aortic arch after the junction of the innominate artery and may cause, when the ascending aorta has a very small diameter, inadequate retrograde flow to the coronary arteries through the ascending aorta. Photiadis et al. [18] performed the Norwood operation with the heart beating using anastomosis of the PTFE tube with innominate artery to rACP without DAC and ascending aortic cannulation using CPB and hypothermia at 18°C.
In this technique variation it is avoided total circulatory arrest and deep hypothermia without aortic clamping, but it is only possible to perform it when the ascending aorta is not extremely hypoplastic in order to allow its cannulation. These authors compared this technique with the use of circulatory arrest with deep hypothermia and demonstrated that, avoiding the use of circulatory arrest, there is significant improvement in hemodynamic performance in the postoperative period, thus reducing hospital mortality. Confirming the current trend of performing the Norwood operation using selective cerebral flow, multicenter study performed by Wernovsky et al. [19] revealed that most of the groups that participated in this study used the rACP. On the other hand, a study using magnetic resonance imaging revealed that there was postoperative neurological disease in 23% of children with HLHS, with worsening or development of new lesions in 73% of patients undergoing rACP [20]. Goldberg et al. [21] performed a clinical study in children undergoing the Norwood procedure and identified delayed psicomotor development and found that the use of rACP has not prevented this complication.
Several changes were performed in the Norwood operation. Poirier et al. [22] modified the reconstruction of the neoaorta and proposed high-flow CPB using phenoxybenzamine to reduce systemic vascular resistance. Another change that resulted in higher stability of the patient in the postoperative period was the anastomosis of the PTFE tube between the right ventricle and the pulmonary arteries or Sano's operation [23]. According to Silva et al. [24], there were no significant difference in mortality in the Norwood operation when Blalock-Taussig shunt and Sano's operation are performed, but there was significant improvement in survival in the second stage when the bidirectional Glenn procedure was performed in the Sano's operation group. The best result in the second stage can be explained by the greater stimulus for growth of central pulmonary arteries when performing the Sano's operation when compared to Blalock-Taussig [25].
In the preoperative approach and operative technique adopted, the immediate postoperative period is also critical in a child with HLHS who had undergone Norwood procedure. The right ventricle has a boundary function and systemic and pulmonary circulations require in parallel precise manipulation of their resistance to provide a QP/QS ratio between 1 and 1.5 to obtain an optimal supply of oxygen to tissues. Monitoring of mixed venous oxygen saturation taken in the right atrium is an important parameter to determine whether it is occurring aerobic or anaerobic metabolism, where this value is less than 30% means anaerobic metabolism and it identifies patients at risk of early mortality. The sudden cardiovascular collapse in the immediate postoperative period in the Norwood procedure is related to increased systemic vascular resistance, increasing cardiac work and oxygen consumption.
The technique proposed herein to correct HLHS is different from all previously described because it associates the rACP with the rRCorP in children with HLHS with HA, avoiding circulatory arrest with deep hypothermia and reducing the time of AC.
CONCLUSIONS
We conclude that the modified Norwood procedure performed in children with HLHS using cardiopulmonary bypass with regional anterograde cerebral perfusion and regional retrograde coronary perfusion avoided circulatory arrest with deep hypothermia and theoretically decreases the time of AC. The immediate surgical outcome was satisfactory without heurological complications, and it is a good option for surgical treatment of high-risk children with HLHS associated with extremely hypoplastic ascending aorta.
REFERENCES
1. Li J, Zhang G, Holtby H, Cai S, Walsh M, Caldarone CA, et al. Significant correlation of comprehensive Aristotle score with total cardiac output during the early postoperative period after the Norwood procedure. J Thorac Cardiovasc Surg. 2008;136(1):123-8. [MedLine]
2. Kilpack VD, Stayer SA, McKenzie ED, Fraser CD Jr, Andropoulos DB. Limiting circulatory arrest using regional low flow perfusion. J Extra Corpor Technol. 2004;36(2):133-8. [MedLine]
3. Jacobs JP, O'Brien SM, Chai PJ, Morell VO, Lindberg HL, Quintessenza JA. Management of 239 patients with hypoplastic left heart syndrome and related malformations from 1993 to 2007. Ann Thorac Surg. 2008;85(5):1691-6.
4. Stasik CN, Gelehrter S, Goldberg CS, Bove EL, Devaney EJ, Ohye RG. Current outcomes and risk factors for the Norwood procedure. J Thorac Cardiovasc Surg. 2006;131(2):412-7. [MedLine]
5. Gaynor JW, Mahle WT, Cohen MI, Ittenbach RF, DeCampli WM, Steven JM, et al. Risk factors for mortality after the Norwood procedure. Eur J Cardiothorac Surg. 2002;22(1):82-9. [MedLine]
6. Wernovsky G, Kuijpers M, Van Rossem MC, Marino BS, Ravishankar C, Dominguez T, et al. Postoperative course in the cardiac intensive care unit following the first stage of Norwood reconstruction. Cardiol Young. 2007;17(6):652-65. [MedLine]
7. Sinzobahamvya N, Photiadis J, Kumpikaite D, Fink C, Blaschczok HC, Brecher AM, et al. Comprehensive Aristotle score: implications for the Norwood procedure. Ann Thorac Surg. 2006;81(5):1794-800. [MedLine]
8. Artrip JH, Campbell DN, Ivy DD, Almodovar MC, Chan KC, Mitchell MB, et al. Birth weight and complexity are significant factors for the management of hypoplastic left heart syndrome. Ann Thorac Surg. 2006;82(4):1252-7.
9. McGuirk SP, Stickley J, Griselli M, Stumper OF, Laker SJ, Barron DJ, et al. Risk assessment and early outcome following the Norwood procedure for hypoplastic left heart syndrome. Eur J Cardiothorac Surg. 2006;29(5):675-81. [MedLine]
10. Delmo Walter EM, Hübler M, Alexi-Meskishvili V, Miera O, Weng Y, Loforte A, et al. Staged surgical palliation in hypoplastic left heart syndrome and its variants. J Card Surg. 2009;24(4):383-91. [MedLine]
11. Ota N, Ikai A, Hirose K, Sakamoto K. Retrospective analysis of stage I Norwood procedures with tricuspid valve insufficiency in the past 5 years. Interact Cardiovasc Thorac Surg. 2007;6(1):121-3. [MedLine]
12. Bove EL, Ohye RG, Devaney EJ, Hirsch J. Tricuspid valve repair for hypoplastic left heart syndrome and the failing right ventricle. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2007:101-4. [MedLine]
13. Kanter KR, Forbess JM, Fyfe DA, Mahle WT, Kirshbom PM. De Vega tricuspid annuloplasty for systemic tricuspid regurgitation in children with univentricular physiology. J Heart Valve Dis. 2004;13(1):86-90. [MedLine]
14. Fantini FA, Gontijo Filho B, Martins C, Lopes RM, Heiden E, Vrandecic E, et al. A operação de Norwood modificada para tratamento da síndrome de hipoplasia do coração esquerdo. Rev Bras Cir Cardiovasc. 2004;19(1):42-6. View article
15. Imoto Y, Kado H, Shiokawa Y, Fukae K, Yasui H. Norwood procedure without circulatory arrest. Ann Thorac Surg. 1999;68(2):559-61. [MedLine]
16. Tchervenkov CI, Chu VF, Shum-Tim D, Laliberte E, Reyes TU. Norwood operation without circulatory arrest: a new surgical technique. Ann Thorac Surg. 2000;70(5):1730-3. [MedLine]
17. Kishimoto H, Kawahira Y, Kawata H, Miura T, Iwai S, Mori T. The modified Norwood palliation on a beating heart. J Thorac Cardiovasc Surg. 1999;118(6):1130-2. [MedLine]
18. Photiadis J, Asfour B, Sinzobahamvya N, Fink C, Schindler E, Brecher AM, et al. Improved hemodynamics and outcome after modified Norwood operation on the beating heart. Ann Thorac Surg. 2006;81(3):976-81. [MedLine]
19. Wernovsky G, Ghanayem N, Ohye RG, Bacha EA, Jacobs JP, Gaynor J W, et al. Hypoplastic left heart syndrome: consensus and controversies in 2007. Cardiol Young. 2007;17(Suppl 2):75-86. [MedLine]
20. Dent CL, Spaeth JP, Jones BV, Schwartz SM, Glauser TA, Hallinan B, et al. Brain magnetic resonance imaging abnormalities after the Norwood procedure using regional cerebral perfusion. J Thorac Cardiovasc Surg. 2006;131(1):190-7. [MedLine]
21. Goldberg CS, Bove EL, Devaney EJ, Mollen E, Schwartz E, Tindall S, et al. A randomized clinical trial of regional cerebral perfusion versus deep hypothermic circulatory arrest: outcomes for infants with functional single ventricle. J Thorac Cardiovasc Surg. 2007;133(4):880-7. [MedLine]
22. Poirier NC, Drummond-Webb JJ, Hisamochi K, Imamura M, Harrison AM, Mee RB. Modified Norwood procedure with a high-flow cardiopulmonary bypass strategy results in low mortality without late arch obstruction. J Thorac Cardiovasc Surg. 2000;120(5):875-84. [MedLine]
23. Sano S, Kawada M, Yoshida H, Kino K, Irie H, Aoki A, et al. Norwood procedure to hypoplastic left heart syndrome. Jpn J Thorac Cardiovasc Surg. 1998;46(12):1311-6. [MedLine]
24. Silva JP, Fonseca L, Baumgratz JF, Castro RM, Franchi SM, Lianza AC, et al. Hypoplastic left heart syndrome: the report of a surgical strategy and comparative results of Norwood x Norwood-Sano approach. Rev Bras Cir Cardiovasc. 2007;22(2):160-8. [MedLine] View article
25. Rumball EM, McGuirk SP, Stümper O, Laker SJ, de Giovanni JV, Wright JG, et al. The RV-PA conduit stimulates better growth of the pulmonary arteries in hypoplastic left heart syndrome. Eur J Cardiothorac Surg. 2005;27(5):801-6. [MedLine]
Article receive on Saturday, June 13, 2009
 All scientific articles published at bjcvs.org are licensed under a Creative Commons license
All scientific articles published at bjcvs.org are licensed under a Creative Commons license













 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket