![]()
![]()
Marcus Vinicius Silva FerreiraI; Cláudio Ribeiro da CunhaI; Gabrielle Santos OliveiraI; Maria Estefânia OttoII; Fernando Antibas AtikI
DOI: 10.21470/1678-9741-2020-0641
ABSTRACT
Introduction: Left ventricular dysfunction after surgical treatment of mitral stenosis is uncommon. We intend to determine the pattern of left ventricular remodeling, shortly after open mitral valve replacement for rheumatic mitral stenosis, with in-hospital postoperative outcomes and the determinants of postoperative worsening of left ventricular ejection fraction.CI = Confidence interval
EF = Ejection fraction
ICU = Intensive care unit
LA = Left atrial
LAV = Left atrial volume
LV = Left ventricular
LVEDD = Left ventricular end-diastolic diameter
LVEDV = Left ventricular end-diastolic volume
LVEF = Left ventricular ejection fraction
LVESD = Left ventricular end-systolic diameter
LVESV = Left ventricular end-systolic volume
MR = Mitral regurgitation
MS = Mitral stenosis
MVA = Mitral valve area
NYHA = New York Heart Association
OR = Odds ratio
PASP = Pulmonary artery systolic pressure
PHT = Pressure half-time
TR = Tricuspid regurgitation
VTILVOT = Velocity-time integral for left ventricle outflow tract
VTIPrMV = Velocity-time integral for mitral valve prosthesis
INTRODUCTION
The hallmark morphology of rheumatic mitral stenosis (MS) results from chronic endocardial insult in rheumatic fever carditis; commissural fusion, thickening, and narrowing of the valve leaflets lead to obstruction of left ventricular (LV) filling(1,2). As opposed to mitral regurgitation, in which LV dysfunction may occur after surgery(3) (as a compensatory mechanism of reduced end-diastolic volume), MS does not hold the same pathophysiological principle.
In MS, reduced stroke volume usually relates to reduced LV preload, rather than ventricular contractile impairment. However, some patients might present true systolic dysfunction that is independent from LV preload(2). The exact mechanism remains unclear, but it is probably multifactorial. Earlier studies found that these patients exhibit larger end-systolic volumes and lower ejection fractions (EF) with rigidity of the LV posterobasal wall at ventriculography(4); a diastolic dysfunction marked by altered ventricular compliance and elevated end-diastolic pressure(5), with preserved EF and normal end-systolic volume(6). Heart failure with reduced or preserved EF in MS has been linked to chronic LV underfilling, endomyocardial fibrosis, subvalvular apparatus rigidity, and elevated right ventricular pressure(4,6-8).
Furthermore, LV remodeling after MS surgery is another critical issue, since knowledge of its pattern in terms of different preoperative echocardiographic parameters can offer a guide on the best timing for intervention. Previous studies(8,9) evaluating MS patients submitted to percutaneous balloon mitral valvuloplasty identified a subgroup of patients with compromised left ventricular ejection fraction (LVEF) that showed no improvement compared to the control group, despite similar increases in mitral valve area (MVA). Although this is not a uniform finding, some authors have hypothesized that the increase in the end-diastolic volume could worsen an underlying dysfunction(10).
The objectives of this study were to determine the pattern of LV remodeling, shortly after open mitral valve replacement for rheumatic MS, with in-hospital postoperative outcomes and the determinants of postoperative worsening of LVEF.
METHODS
Patients
From January 2008 to January 2015, 107 adult patients with pure rheumatic MS or mixed lesions with predominant MS were submitted to primary open mitral valve replacements, associated or not with tricuspid valve repairs and/or Cox-maze procedures. Exclusion criteria included more than moderate mitral regurgitation, aortic valve pathology, previous cardiac surgery, patients submitted to mitral valve repair, and those with incomplete follow-up.
Data were retrieved in part from the prospective cardiovascular surgery registry and in part from each electronic patient’s medical record. All echocardiographic analysis was performed in our institution by a team of qualified physicians following strict standardized protocols. Routine periodic interobserver variability is tested in our laboratory. Echocardiographic data were obtained from the echocardiography laboratory records. These data were approved by the Institutional Review Board (Ethics Committee approval number 2.644.241), which approved their use for research purposes with patient consent waived.
Operations were performed with normothermic cardiopulmonary bypass and hypothermic antegrade and retrograde blood cardioplegia for myocardial protection. Mitral valve replacement was performed with partial preservation of the subvalvular apparatus. The anterior leaflet was systematically resected. The posterior leaflet was preserved entirely or partially resected, in order avoid interference with the movement of the prosthesis leaflets and with LV filling. Secondary chordae were resected where extensive fibrotic tissue foreshortened the subvalvular apparatus, in addition to papillary muscle splitting to allow better ventricular filling. All calcified leaflet tissue was routinely removed. There were no patients in this series with mitral annular calcification in need of decalcification and reconstruction of the posterior atrioventricular groove.
Echocardiographic Examination
All patients were submitted to a comprehensive two-dimensional and Doppler echocardiogram (HDI 5000, Philips ATL, Bothell, WA; HD 7, Philips, Koninklijke, N.V.; Vivid E9, GE) using 2/4 MHz transducer and second harmonic imaging, before and after any cardiothoracic surgical procedure in our unit. For the purpose of this research, the closest examinations performed before and after the surgery were reviewed. All postoperative examinations were completed prior to patient discharge.
LVEF was determined by the Simpson method. Left atrial volume (LAV) was calculated by the modified Simpson method and indexed to body surface areas. LAV was measured in the frame just before mitral valve opening, excluding the left atrial appendage and pulmonary veins.
MVA was measured by the planimetry method, using a parasternal short-axis view and pressure half-time (PHT), complying with the American Society of Echocardiography Guidelines(11). Mean mitral valve diastolic gradients were measured by pulsed-wave Doppler. After valve replacement, patients were additionally evaluated for PHT and Doppler velocity index.
Definitions of Study Groups and Outcomes
LV remodeling was studied through changes in LV dimensions, volumes, and function shortly after mitral valve replacement. For the purpose of this study, worsening of LV function was defined by a decrease in the LVEF of 10% or more between preoperative and postoperative echocardiographies. These criteria were based on the latest guidelines issued by the American Society of Echocardiography and the European Association of Cardiovascular Imaging(12), which establishes a standard deviation of five absolute points for the mean normal values of LVEF, for both genders. That difference of > 10% was validated because it is greater than the interobserver accepted assessment error that may occur in echocardiography.
The outcomes assessed included intraoperative support (myocardial ischemic time, cardiopulmonary bypass time), as well as postoperative in-hospital mortality and morbidity rates (defined in accordance with the Society of Thoracic Surgeons National Database, available from: http://www.sts.org/registries-research-center/sts-national-database/adult-cardiac-surgery-database/data-collection).
Data Analyses
All statistical analyses were performed using IBM Corp. Released 2016, IBM SPSS Statistics for Windows, Version 24.0, Armonk, NY: IBM Corp. Categorical variables are summarized as frequencies and percentages. The distribution patterns of variables were determined by the Kolmogorov-Smirnov test. Continuous variables are summarized as means and standard deviation when normally distributed or as medians with interquartile range when the data is skewed.
Categorical outcomes were compared using either χ2 or Fisher’s exact test (with less than five observations). Continuous outcomes were compared either by parametric tests (Student’s t-test) when variables had normal distribution, or by non-parametric tests (Mann-Whitney and Wilcoxon) when variable distribution was skewed. To compare temporal pattern of postoperative echocardiographic indices of dimensions and function across time, all repeated continuous values were analyzed longitudinally using repeated measures analyses of variance. Clinical and echocardiographic variables related to the development of postoperative worsening of LV function were determined by multivariable logistic regression. First, we determined factors associated with postoperative worsening of LV function using a univariable model. Variable selection, with a P-value criterion of 0.2 for retention of variables in the model, was followed by variable storage using automated forward selection and backward elimination. Receiver operating characteristic curves were obtained and the area under the curve was determined. A P-value of 0.05 was considered statistically significant.
RESULTS
Overall, there was a marked predominance of women (N=93, 86.9%), and the mean age was 45±11 years (range from 22 to 71 years). More than half of the population had preoperative atrial fibrillation and they were in New York Heart Association (NYHA) functional class III or IV (Table 1). Mitral valve replacement was performed under mean cardiopulmonary bypass time of 93.7±29 minutes and mean cross-clamping time of 76±24.1 minutes, including associated procedures when applicable. Patients that presented with worsening EF after the procedure were those with lower preoperative body weight (P<0.01), that determined lower body mass index (P<0.01) and body surface area (P<0.01).
| Total (N = 107) |
Preserved EF (N = 89) |
Worsening EF (N = 18) |
P-value | |
|---|---|---|---|---|
| Gender (male) | 14 (13.1%) | 13 (14.6%) | 1 (5.6%) | 0.54 |
| Age‡ | 48 (38 - 53) | 48 (39 - 53) | 48 (33.7 - 59) | 0.93 |
| Weight (kg)† | 61.6 ± 12.2 | 63.4 ± 12.1 | 52.9 ± 8.5 | < 0.01 |
| Height (m)‡ | 1.57 (1.54 - 1.62) | 1.57 (1.54 - 1.63) | 1.55 (1.50 - 1.61) | 0.15 |
| Body surface area‡ | 1.61 (1.52 - 1.72) | 1.63 (1.54 - 1.74) | 1.51 (1.43 - 1.57) | < 0.01 |
| Body mass index† | 24.5 ± 4.8 | 25.1 ± 4.9 | 21.6 ± 3.2 | < 0.01 |
| NYHA Class III or IV | 58 (54.2%) | 47 (55.3%) | 11 (68.8%) | 0.41 |
| Hypertension | 26 (24.3%) | 23 (25.8%) | 3 (16.7%) | 0.55 |
| Diabetes mellitus | 6 (5.6%) | 6 (6.7%) | 0 | 0.59 |
| Hyperlipidemia | 6 (5.6%) | 6 (6.7%) | 0 | 0.59 |
| Previous or current smoking | 32 (29.9%) | 27 (30.7%) | 5 (27.8%) | > 0.999 |
| Coronary artery disease | 4 (3.7%) | 3 (3.4%) | 1 (5.6%) | 0.53 |
| Previous myocardial infarction | 3 (2.8%) | 2 (2.2%) | 1 (5.6%) | 0.43 |
| Previous stroke | 10 (9.3%) | 8 (9%) | 2 (11.1%) | 0.67 |
| Atrial fibrillation | 54 (50.5%) | 44 (49.4%) | 10 (55.6%) | 0.8 |
Intraoperative variables did not differ among study groups. Those include the type of prosthesis used (bioprosthesis in 59.1% of preserved EF group vs. 72.2% of worsening EF group; P=0.4), its sizing (28±1.9 vs. 27.3±1.4; P=0.2), presence of concomitant procedures - Maze procedure and/or tricuspid repair (43% vs. 44.4%; P=0.2) -, and duration of cardiopulmonary bypass time (94.2±28.3 minutes vs. 91.3±33.1 minutes; P=0.6) and aortic cross-clamping time (76.1±23.3 minutes vs. 75.3±28.2 minutes; P=0.8).
Pattern of Ventricular Remodeling
Postoperatively (Table 2), there was an increase in LV dimensions and volumes, due to greater ventricular filling and relief of obstruction at mitral valve level, with decreased LAV and pulmonary artery pressures. Although the overall change in LVEF was significant (66.6% to 63.2%, P<0.01), its means were in the normal range. Worsening of LVEF > 10% occurred in 18 patients (16.8%) and only six patients (5.6%) presented EF < 50%.
| Preserved EF (N = 89) |
Worsening EF (N = 18) |
Total (N = 107) |
|||||||
|---|---|---|---|---|---|---|---|---|---|
| Preoperative‡ | Postoperative‡ | P-value | Preoperative‡ | Postoperative‡ | P-value | Preoperative‡ | Postoperative‡ | P-value | |
| Indexed LVEDD (mm/m2) |
27.3 (25.2 - 29.4) | 27.9 (26.2 - 29.8) | < 0.01 | 28.2 (24.6 - 31.2) | 29.6 (26.3 - 33.5) | 0.10 | 27.5 (24.8 - 29.5) | 27.9 (26.2 - 30.32) | < 0.01 |
| Indexed LVESD (mm/m2) |
17.6 (16.1 - 19.0) | 18.1 (16.0 - 19.3) | 0.03 | 16.8 (14.2 - 18.7) | 19.4 (18.4 - 24.5) | < 0.01 | 17.4 (15.8 - 18.9) | 18.3 (16.2 - 19.6) | < 0.01 |
| Indexed LVEDV (ml/m2) |
57.3 (45.8 - 66.8) | 58.7 (50.8 - 67.9) | < 0.01 | 52.2 (39.8 - 62.8) | 62.8 (49.4 - 75.0) | 0.05 | 57.1 (45.1 - 66.2) | 58.7 (50.5 - 68.5) | < 0.01 |
| Indexed LVESV (ml/m2) |
20.3 (15.1 - 22.9) | 20.7 (16.2 - 24.4) | 0.05 | 16.3 (10.2 - 20.3) | 23.5 (19.6 - 39.2) | < 0.01 | 19.4 (14.9 - 22.8) | 20.9 (16.8 - 26.8) | < 0.01 |
| LVEF (%) | 64.4 (61.6 - 68.5) | 65.3 (61.0 - 69.1) | 0.58 | 71.7 (65.5 - 79.0) | 58.4 (33.9 - 62.4) | < 0.01 | 65.8 (62.1 - 68.7) | 64 (59.8 - 68.5) | 0.02 |
| Indexed LA volume (ml/m2) |
61.3 (50.5 - 73.7) | 45.6 (40.0 - 55.6) | < 0.01 | 63.7 (48.8 - 81.8) | 53.3 (39.3 - 78.1) | < 0.01 | 62.5 (50.5 - 74.2) | 46 (40 - 56.4) | < 0.01 |
| Mean mitral gradient (mmHg) |
12.0 (8.5 - 17.0) | 6.2 (4.1 - 8.1) | < 0.01 | 15.5 (11.7 - 19.2) | 6.0 (3.8 - 8.2) | < 0.01 | 13.0 (9 - 18) | 6.0 (4.0 - 8.0) | < 0.01 |
| PASP (mmHg) |
50.0 (40.0 - 62.0) | 38.0 (35.0 - 47.5) | < 0.01 | 52.0 (43.0 - 83.0) | 48.0 (34.5 - 55.5) | 0.08 | 51.5 (40 - 62) | 39.0 (35.0 - 49.5) | < 0.01 |
‡ Median (interquartile range)
EF=ejection fraction; LA=left atrial; LVEDD=left ventricular end-diastolic diameter; LVEDV=left ventricular end-diastolic volume; LVEF=left ventricular ejection fraction; LVESD=left ventricular end-systolic diameter; LVESV=left ventricular end-systolic volume; PASP=pulmonary artery systolic pressure

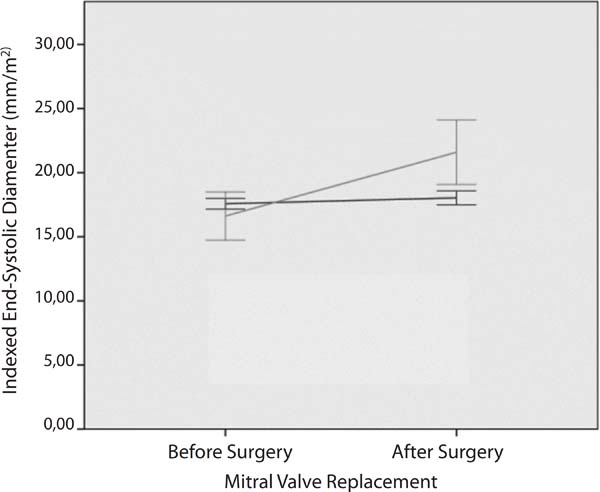
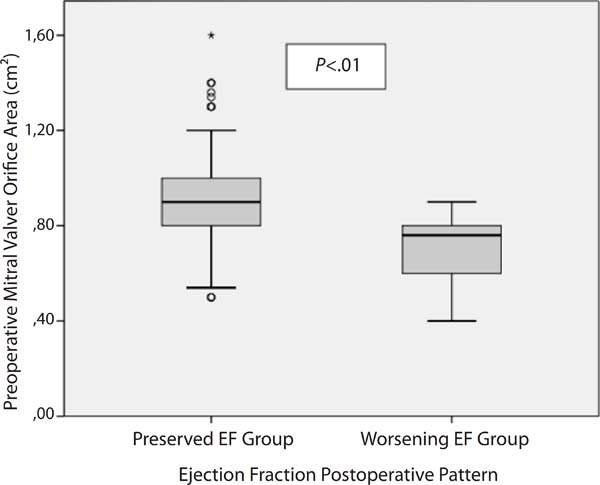
When the groups were compared (Table 3), LV end-diastolic diameters (F=0.04; P=0.83) and volumes (F=0.75; P=0.38) increased similarly. The increase in the end-systolic volume (F=34; P<0.01), as shown in Figure 1, and diameter (F=43.1; P<0.01) was far greater in the group that presented worsening of EF. Moreover, the mitral valve orifice area (Figure 2) was smaller in the group with deteriorated EF, indicating a more severe MS. Obstruction relief postoperatively was greater in the same group (F=4.5; P=0.03). Both groups presented similar decreases in LAV (F=23.9; P=0.2) and proportional improvements in pulmonary artery systolic pressures (F=0.38; P=0.53).
| Preoperative | Postoperative | |||||||
|---|---|---|---|---|---|---|---|---|
| Total (N = 107) |
Preserved EF (N = 89) |
Worsening EF (N = 18) |
P-value | Total (N = 107) |
Preserved EF (N = 89) |
Worsening EF (N = 18) |
P-value | |
| Indexed LVEDD (mm/m2)‡ |
27.5 (24.8 - 29.5) | 27.3 (25.2 - 29.4) | 28.2 (24.6 - 31.2) | 0.48 | 27.9 (26.2 - 30.32) | 27.9 (26.2 - 29.8) | 29.6 (26.3 - 33.5) | 0.05 |
| Indexed LVESD (mm/m2)‡ |
17.4 (15.8 - 18.9) | 17.6 (16.1 - 19.0) | 16.8 (14.2 - 18.7) | 0.18 | 18.3 (16.2 - 19.6) | 18.1 (16.0 - 19.3) | 19.4 (18.4 - 24.5) | < 0.01 |
| Indexed LVEDV (ml/m2)‡ |
57.1 (45.1 - 66.2) | 57.3 (45.8 - 66.8) | 52.2 (39.8 - 62.8) | 0.40 | 58.7 (50.5 - 68.5) | 58.7 (50.8 - 67.9) | 62.8 (49.4 - 75.0) | 0.5 |
| Indexed LVESV (ml/m2)‡ |
19.4 (14.9 - 22.8) | 20.3 (15.1 - 22.9) | 16.3 (10.2 - 20.3) | 0.01 | 20.9 (16.8 - 26.8) | 20.7 (16.2 - 24.4) | 23.5 (19.6 - 39.2) | 0.03 |
| LVEF (%)‡ | 65.8 (62.1 - 68.7) | 64.4 (61.6 - 68.5) | 71.7 (65.5 - 79.0) | < 0.01 | 64.04 (59.8 - 68.5) | 65.3 (61.0 - 69.1) | 58.4 (33.9 - 62.4) | < 0.01 |
| Indexed LA volume (ml/m2)‡ |
62.5 (50.5 - 74.2) | 61.3 (50.5 - 73.7) | 63.7 (48.8 - 81.8) | 0.73 | 46.0 (40.0 - 56.4) | 45.6 (40.0 - 55.6) | 53.3 (39.3 - 78.1) | 0.17 |
| Mean mitral gradient (mmHg)‡ |
13.0 (9.0 - 18.0) | 12.0 (8.5 - 17.0) | 15.5 (11.7 - 19.2) | 0.02 | 6.0 (4.0 - 8.0) | 6.2 (4.1 - 8.1) | 6.0 (3.8 - 8.2) | 0.65 |
| MVA (cm2)‡ | 0.80 (0.70 - 0.99) | 0.9 (0.8 - 1.0) | 0.76 (0.60 - 0.80) | < 0.01 | - | - | - | - |
| Indexed MVA (cm2/m2)‡ |
0.52 (0.44 - 0.61) | 0.52 (0.45 - 0.62) | 0.49 (0.40 - 0.54) | 0.08 | - | - | - | - |
| Wilkins-Block‡ | 10.0 (9.0 - 11.0) | 10 (9.0 - 11.0) | 11.0 (10.0 - 12.0) | 0.05 | - | - | - | - |
| PHT (ms)‡ | - | - | - | - | 72.0 (52.0 - 100.0) | 71.0 (51.7 - 95.0) | 75 (60.5 - 245.5) | 0.36 |
| VTIPrMV/VTILVOT† | - | - | - | - | 1.9 ± 0.5 | 2.0 ± 0.5 | 1.9 ± 0.5 | 0.74 |
| PASP (mmHg)‡ | 51.5 (40.0 - 62.0) | 50.0 (40.0 - 62.0) | 52.0 (43.0 - 83.0) | 0.27 | 39.0 (35.0 - 49.5) | 38.0 (35.0 - 47.5) | 48.0 (34.5 - 55.5) | 0.06 |
| Moderate MR | 37 (34.6%) | 30 (33.7%) | 7 (38.9%) | 0.79 | - | - | - | - |
| Moderate or severe TR |
26 (24.3%) | 19 (21.3%) | 7 (38.9%) | 0.14 | - | - | - | - |
‡ Median (interquartile range)
† Mean (95% confidence interval)
EF=ejection fraction; LA=left atrial; LVEDD=left ventricular end-diastolic diameter; LVEDV=left ventricular end-diastolic volume; LVEF=left ventricular ejection fraction; LVESD=left ventricular end-systolic diameter; LVESV=left ventricular end-systolic volume; MR=mitral regurgitation; MVA=mitral valve area; PASP=pulmonary artery systolic pressure; PHT=pressure half-time; TR=tricuspid regurgitation; VTILVOT=velocity-time integral for left ventricle outflow tract; VTIPrMV=velocity-time integral for mitral valve prosthesis


Determinants of Worsening of Left Ventricular Ejection Fraction
Body weight (P=0.005; odds ratio [OR]=0.89) and MVA (P=0.02; OR=0.02) were identified as independent predictors of worsening of LVEF. Moderate mitral regurgitation was not associated with worsening of postoperative EF.
A receiver operating characteristic curve was then obtained for the MVA by planimetry. Regarding the non-indexed MVA, the optimal cutoff for prognostic value was determined by the model as 0.8 (sensitivity=88.2%, specificity=54.4%), with an overall area under the curve of 0.752 (95% confidence interval 0.645 - 0.859; P<0.01).
Surgical Outcomes
Postoperative in-hospital morbidity and mortality rates are depicted in Table 4. Patients in the group with worsening LVEF presented higher mortality rates, more prolonged mechanical ventilation and nosocomial pneumonia, and prolonged hospital and intensive care unit lengths of stay. Postoperatively, this group developed more frequently hemodynamic instability with elevated filling pressures. Causes of death of this group were cardiogenic shock in all three patients.
| Total (N = 107) |
Preserved EF (N = 89) |
Worsening EF (N = 18) |
OR (95% CI) | P-value | |
|---|---|---|---|---|---|
| In-hospital mortality | 4 (3.7%) | 1 (1.1 %) | 3 (16.7%) | 17.6 (1.7 - 181) | 0.01 |
| Stroke | 0 | 0 | 0 | - | - |
| Myocardial infarction | 0 | 0 | 0 | - | - |
| Acute renal failure | 7 (6.5%) | 4 (4.5%) | 3 (16.7%) | 4.2 (.8 - 20.7) | 0.08 |
| New-onset atrial fibrillation | 19 (17.7%) | 18 (20.5%) | 1 (5.6%) | .23 (.02 - 1.83) | 0.16 |
| Prolonged mechanical ventilation | 5 (4.6%) | 1 (1.1%) | 4 (22.2%) | 24.8 (2.6 - 238) | <0.01 |
| Nosocomial pneumonia | 5 (4.6%) | 2 (2.3%) | 3 (16.7%) | 8.6 (1.3 - 55.8) | 0.03 |
| ICU length of stay (days)‡ | 4 (2 - 5) | 3 (2 - 3) | 6 (3 - 8) | - | 0.03 |
| Hospital length of stay (days)‡ | 13 (9 - 17) | 12 (9 - 17) | 15 (11 - 18) | - | 0.04 |
‡ Median (interquartile range)

DISCUSSION
This study shows that there are different patterns of LV remodeling postoperatively among patients with rheumatic MS submitted to open mitral valve replacement. Worsening LVEF > 10% is uncommon, but when present may lead to higher morbidity and mortality rates. Predictors of worsening LVEF relate to a specific subset of patients with lower body weight and smaller mitral valve orifice areas.
Patient profiles showed a predominance of women in their forties presenting as very symptomatic (nearly half in NYHA functional class > III) and about half with preoperative atrial fibrillation. Patients submitted to mitral valve repair were excluded since this could be a confounder when analyzing LV remodeling patterns.
The pattern of ventricular remodeling in patients presenting with worsening of LVEF was associated with greater ventricular dilatation. Moreover, they also had smaller preoperative mitral valve orifice areas, indicating more severe MS at presentation. This finding might be related to poor adaptation by the left ventricle to a subtle increase in end-diastolic volumes. Diastolic dysfunction is usually the explanation for that (13), but underlying systolic dysfunction could be unmasked after surgery. LVEF has limitations for defining the degree of systolic ventricular dysfunction(14). Echocardiographic assessment with speckle tracking echocardiography has demonstrated that longitudinal and circumferential strain rates are globally diminished in MS patients(15), even with preserved EF.
Lower body weight and smaller preoperative mitral valve orifice areas were related to worsening of LVEF postoperatively. The association between severity of MS and ventricular dysfunction is conflictive. Previous studies have shown a linear relationship between MVA in severe MS patients and systolic and diastolic myocardial velocities determined by Doppler tissue imaging(16),(17). Moreover, a positive correlation was found between MVA and impaired longitudinal strain rates(18). However, these results are not consistent in patients with mild to moderate MS(15,19).
The 2014 American Heart Association/American College of Cardiology Guidelines(20) on valvular heart disease recommend that the presence of symptoms with evidence of severe MS (MVA < 1.5 cm2, stage D) is necessary as an indication for surgery. It is also considered reasonable as an indication for percutaneous balloon valvuloplasty (rather than surgery) a Recommendation Class IIa in asymptomatic patients with very severe MS (MVA < 1.0 cm2, stage C) and favorable morphology, in the absence of contraindications. This recommendation stresses the incremental risk of very severe MS (MVA < 1.0 cm2) over severe stenosis (MVA < 1.5 cm2), even in stage C patients. The 2017 European Society of Cardiology/European Association for Cardio-Thoracic Surgery Guidelines(21) on valvular disease recommend as an indication that intervention in asymptomatic patients be performed only percutaneously, with high thromboembolic risk and/or high risk of hemodynamic decompensation, at the same recommendation level as the American guidelines. The Brazilian Society of Cardiology Guidelines(22) recommend intervention as Class IIa in asymptomatic patients, only in the presence of pulmonary hypertension and/or new-onset atrial fibrillation, if not suitable for percutaneous balloon valvuloplasty. Our data supports this indication for surgery based on symptoms alone or with complicating factors (new-onset atrial fibrillation, pulmonary hypertension, or desire for pregnancy) that may be misleading, particularly when MVA < 1.0 cm2.
Our data showed that worsening of LVEF > 10% is associated with poorer in-hospital outcomes. Similarly, proper assessment of LV systolic and diastolic function is important for determining surgical risk and prognosis. Early intervention seems reasonable for this patient subset. In our study, MVA of 0.80 cm2 presented good sensitivity (88.2%) and low specificity (54.4%), raising concerns about very severe MS and postoperative subclinical ventricular dysfunction.
Limitations
This is a retrospective patient cohort study, with its inherent limitations. The low number of events curtailed a more appropriate analysis of outcomes with multivariable logistic regression, particularly those that achieve worsening LVEF (N=19). However, a fair number of rheumatic MS patients were included. The importance of this study lies in the recognition that there is a subset of patients who develop clinically relevant LV adverse remodeling. Long-term clinical and echocardiographic data would be extremely important for understanding whether ventricular remodeling pattern persists over time, together with its impact on survival.
CONCLUSION
LV remodeling patterns differed among patients with predominant rheumatic MS undergoing open mitral valve replacement. Lower preoperative body weight and MVA were independent determinants of deteriorating EF with increased end-systolic volumes, indicating that this specific problem may occur in anthropometric smaller patients with more extensive rheumatic disease.
REFERENCES
1. Remenyi B, ElGuindy A, Smith SC Jr, Yacoub M, Holmes DR Jr. Valvular aspects of rheumatic heart disease. Lancet. 2016;387(10025):1335-46.
2. Chandrashekhar Y, Westaby S, Narula J. Mitral stenosis. Lancet. 2009;374(9697):1271-83.
3. Gillam LD, Schwartz A. Primum non nocere: the case for watchful waiting in asymptomatic "severe" degenerative mitral regurgitation. Circulation. 2010;121(6):813-21; discussion 821.
4. Heller SJ, Carleton RA. Abnormal left ventricular contraction in patients with mitral stenosis. Circulation. 1970;42(6):1099-110.
5. Eleid MF, Nishimura RA, Lennon RJ, Sorajja P. Left ventricular diastolic dysfunction in patients with mitral stenosis undergoing percutaneous mitral balloon valvotomy. Mayo Clin Proc. 2013;88(4):337-44.
6. Liu CP, Ting CT, Yang TM, Chen JW, Chang MS, Maughan WL, et al. Reduced left ventricular compliance in human mitral stenosis. Role of reversible internal constraint. Circulation. 1992;85(4):1447-56.
7. Klein AJ, Carroll JD. Left ventricular dysfunction and mitral stenosis. Heart Fail Clin. 2006;2(4):443-52.
8. Lee TM, Su SF, Chen MF, Liau CS, Lee YT. Changes of left ventricular function after percutaneous balloon mitral valvuloplasty in mitral stenosis with impaired left ventricular performance. Int J Cardiol. 1996;56(3):211-5.
9. Yasuda S, Nagata S, Tamai J, Ishikura F, Yamabe T, Kimura K, et al. Left ventricular diastolic pressure-volume response immediately after successful percutaneous transvenous mitral commissurotomy. Am J Cardiol. 1993;71(11):932-7.
10. Razzolini R, Ramondo A, Isabella G, Cardaioli P, Campisi F, De Leo A, et al. Acute changes in left ventricular function after percutaneous transluminal mitral valvuloplasty. Heart Vessels. 1996;11(2):86-91.
11. 11. Baumgartner H, Hung J, Bermejo J, Chambers JB, Evangelista A, Griffin BP, et al. Echocardiographic assessment of valve stenosis: EAE/ASE recommendations for clinical practice. J Am Soc Echocardiogr. 2009;22(1):1-23; quiz 101-2. Erratum in: J Am Soc Echocardiogr. 2009;22(5):442.
12. Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American society of echocardiography and the European association of cardiovascular imaging. J Am Soc Echocardiogr. 2015;28(1):1-39.e14.
13. Kovács Á, Papp Z, Nagy L. Causes and pathophysiology of heart failure with preserved ejection fraction. Heart Fail Clin. 2014;10(3):389-98.
14. Cikes M, Solomon SD. Beyond ejection fraction: an integrative approach for assessment of cardiac structure and function in heart failure. Eur Heart J. 2016;37(21):1642-50.
15. Yıldırımtürk Ö, Helvacıoğlu FF, Tayyareci Y, Yurdakul S, Aytekin S. Subclinical left ventricular systolic dysfunction in patients with mild-to-moderate rheumatic mitral stenosis and normal left ventricular ejection fraction: an observational study. Anadolu Kardiyol Derg. 2013;13(4):328-36.
16. Ozdemir K, Altunkeser BB, Gök H, Içli A, Temizhan A. Analysis of the myocardial velocities in patients with mitral stenosis. J Am Soc Echocardiogr. 2002;15(12):1472-8.
17. Erturk M, Aksu HU, Celik O, Uzun F, Akgul O, Pusuroglu H, et al. Evaluation of the effect of mitral stenosis severity on the left ventricular systolic function using isovolumic myocardial acceleration. Cardiol J. 2014;21(4):442-8.
18. Bilen E, Kurt M, Tanboga IH, Kaya A, Isik T, Ekinci M, et al. Severity of mitral stenosis and left ventricular mechanics: a speckle tracking study. Cardiology. 2011;119(2):108-15.
19. Ozdemir AO, Kaya CT, Ozcan OU, Ozdol C, Candemir B, Turhan S, et al. Prediction of subclinical left ventricular dysfunction with longitudinal two-dimensional strain and strain rate imaging in patients with mitral stenosis. Int J Cardiovasc Imaging. 2010;26(4):397-404.
20. Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP 3rd, Guyton RA, et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: executive summary: a report of the American college of cardiology/American heart association task force on practice guidelines. Circulation. 2014;129(23):2440-92. Erratum in: Circulation. 2014;129(23):e650.
21. Baumgartner H, Falk V, Bax JJ, De Bonis M, Hamm C, Holm PJ, et al. 2017 ESC/EACTS guidelines for the management of valvular heart disease. Eur Heart J. 2017;38(36):2739-91.
22. Tarasoutchi F, Montera MW, Ramos AIO, Sampaio RO, Rosa VEE, Accorsi TAD, et al. Update of the Brazilian guidelines for valvular Heart Disease - 2020. Arq Bras Cardiol. 2020 Oct;115(4):720-775. English, Portuguese.
Authors' roles & responsibilities
MVSF Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved; final approval of the version to be published
CRC Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved; final approval of the version to be published
GSO Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved; final approval of the version to be published
MEO Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved; final approval of the version to be published
FAA Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved; final approval of the version to be published
Article receive on Sunday, November 15, 2020
Article accepted on Monday, January 4, 2021
 All scientific articles published at bjcvs.org are licensed under a Creative Commons license
All scientific articles published at bjcvs.org are licensed under a Creative Commons license













All rights reserved 2017 / © 2024 Brazilian Society of Cardiovascular Surgery
DEVELOPMENT BY ![]()

 English PDF
English PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket