![]()
![]()
Sérgio C. RayolI; Michel Pompeu B. O. SáI; Luiz Rafael P. CavalcantiI; Roberto G. S. DinizI; Álvaro M. PerazzoI; Antônio C. A. EscorelI; Konstantin ZhigalovIV; Arjang RuhparwarIV; Alexander WeymannIV; Ricardo C. LimaI
DOI: 10.21470/1678-9741-2019-0373
ABSTRACT
Objective: To test the German Aortic Valve (GAV) score at our university hospital in patients undergoing isolated aortic valve replacement (AVR).AUC = Area under the ROC curve
AVR = Aortic valve replacement
CI = Confidence interval
COPD = Chronic obstructive pulmonary disease
EuroSCORE = European System for Cardiac Operative Risk Evaluation
GAV = German Aortic Valve
LR = Likelihood ratio
LVEF = Left ventricular ejection fraction
NYHA = New York Heart Association
ROC = Receiver operating characteristic
SPSS = Statistical Package for the Social Sciences
TAVI = Transcatheter aortic valve implantation
INTRODUCTION
The assessment of operative risk is mandatory for all cardiac procedures, since patients need to be informed preoperatively about the risks and surgeons must weigh up pros and cons of a certain procedure. In this scenario, risk scoring systems are used to predict and evaluate results.
Although there are widely spread risk scores, such as the European System for Cardiac Operative Risk Evaluation (EuroSCORE)[1], that have demonstrated good predictive accuracy in the field of cardiovascular surgery, the trend of the moment is for more specific scores to be applied to more specific contexts in cardiac surgery.
Könning et al.[2] published in 2013 the German Aortic Valve (GAV) score. It was designed for fair and reliable outcome evaluation, allows comparison of predicted and observed mortality for conventional aortic valve replacement (AVR) and transcatheter aortic valve implantation (TAVI) in low-, moderate-, and high-risk groups, enables a risk-adjusted benchmark of outcome, and fosters the efforts for continuous improvement of quality in aortic valve procedures.
Since the score has never been tested in Brazil, we aimed to validate the GAV score in patients who underwent conventional AVR at a Brazilian center.
METHODS
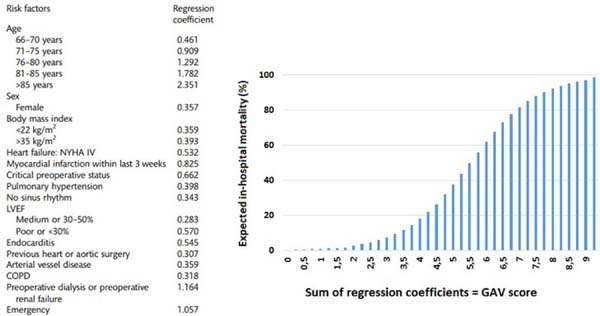
Patients who underwent conventional AVR between January 2015 and December 2018 were included in the study. Those who underwent concomitant procedures or TAVI were excluded. Data were collected and analyzed retrospectively. Primary endpoint was in-hospital mortality. Patients’ GAV scores were calculated according to the criteria described by Kötting et al.[2] (Figure 1). The score is calculated through the sum of regression coefficients, which corresponds to a certain expected operative mortality.
COPD=chronic obstructive pulmonary disease; LVEF=left ventricular
ejection fraction; NYHA=New York Heart Association

COPD=chronic obstructive pulmonary disease; LVEF=left ventricular
ejection fraction; NYHA=New York Heart Association
Sensitivity and specificity were assessed through the receiver operating characteristic (ROC) curve. The discrimination measures the capacity of a model (in this case, the GAV score) to differentiate between the individuals of a sample who suffer an event (in this case, death) from those who do not. The discriminative capacity of the model was estimated by means of the area under the ROC curve (AUC). Calibration of the GAV score was assessed by the Hosmer-Lemeshow test. The calibration is considered to be poor if the test is statistically significant. For the analysis, the Statistical Package for the Social Sciences (SPSS)® software (SPSS, Inc., Chicago, IL, United States of America), version 15.0, for Windows® was used. P-values < 0.05 were considered statistically significant.
RESULTS
We evaluated 224 isolated AVR procedures in adult patients. The mortality rate was 8.04% (18 patients). The patients’ mean age was 58.2±19.3 years and 25% of them were female (56 patients).
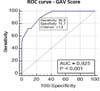
Mean GAV score was 1.73±5.86 (min: 0.0; max: 3.53). The GAV score showed excellent discriminative capacity (AUC 0.925, 95% confidence interval [CI] 0.882-0.956; P<0.001) (Figure 2). The calibration of the model was tested by the Hosmer-Lemeshow method. The derived P-value of 0.687 confirmed a valid accordance of predicted and observed mortality, which means good calibration of the model.
The cutoff “1.8”turned out to be the best discriminatory point with the best combination of sensitivity (88.9%) and specificity (75.7%) to predict operative death (Table 1).
| Score | Sensitivity | 95% CI | Specificity | 95% CI | +LR | -LR |
|---|---|---|---|---|---|---|
| ≥ 0.4 | 100 | 81.5 - 100 | - | 0.0 - 1.8 | 1 | |
| > 1.1 | 100 | 81.5 - 100 | 57.77 | 50.7 - 64.6 | 2.37 | - |
| > 1.4 | 94.44 | 72.7 - 99.9 | 67.96 | 61.1 - 74.3 | 2.95 | 0.082 |
| > 1.8 | 88.89 | 65.3 - 98.6 | 75.73 | 69.3 - 81.4 | 3.66 | 0.15 |
| > 2.3 | 72.22 | 46.5 - 90.3 | 87.38 | 82.1 - 91.6 | 5.72 | 0.32 |
| > 2.9 | 72.22 | 46.5 - 90.3 | 91.26 | 86.5 - 94.7 | 8.27 | 0.30 |
| > 3.7 | 55.56 | 30.8 - 78.5 | 99.03 | 96.5 - 99.9 | 57.22 | 0.45 |
| > 4.7 | 50 | 26 - 74 | 100 | 98.2 - 100 | 0.50 | |
| > 11.9 | - | 0.0 - 18.5 | 100 | 98.2 - 100 | 1 |

DISCUSSION
The presumption that a scoring system might be comprehensive enough for all patients and cardiovascular surgical procedures could not be further from the truth[3,4]. For instance, the widely used EuroSCORE was based on a data set consisting mainly of coronary artery bypass surgeries. Thus, such score might be less well adapted to aortic procedures than a specific score as the one evaluated in the present study. Such aspects have been highlighted by other authors as well[5-8].
Kalender et al.[9] tested for the first time the GAV score out of Germany, studying only 35 isolated AVR procedures in adult patients in Turkey. The patients’ mean age was 61.14±13.25 years (range 29-80 years). The number of female patients was 14 (40%). Mean GAV score was 1.05±0.96 (min: 0; max: 4.98) and mean EuroSCORE II was 2.30±2.60 (min: 0.62, max: 2.30). The GAV score scale showed modest discriminative capacity (AUC 0.647, 95% CI 0.439-0.854).
To the best of our knowledge, our study is the first one to report the results of the GAV score in a Latin American scenario. It is well known that predictive models work best in the series at the location where it was developed. For this reason, the GAV score fits best to the population in Germany. Nevertheless, despite the differences between German and Brazilian populations, the score also showed a very good discriminative capacity in our population.
REFERENCES
1. Nashef SA, Roques F, Sharples LD, Nilsson J, Smith C, Goldstone AR, et al. EuroSCORE II. Eur J CardiothoracSurg. 2012;41(4):734-44; discussion 744-5. doi:10.1093/ejcts/ezs043.
2. Kötting J, Schillerb W, Beckmann A, Schäfer E, Döbler K, Hamm C, et al. German aortic valve score: a new scoring system for prediction of mortality related to aortic valve procedures in adults. Eur J Cardiothorac Surg. 2013;43(5):971-7. doi:10.1093/ejcts/ezt114.
3. Hannan EL, Wu C, Bennett EV, Carlson RE, Culliford AT, Gold JP, et al. Risk index for predicting in-hospital mortality for cardiac valve surgery. Ann Thorac Surg. 2007;83(3):921-9. doi:10.1016/j.athoracsur.2006.09.051.
4. Zheng Z, Li Y, Zhang S, Hu S; Chinese CABG Registry Study. The Chinese coronary artery bypass grafting registry study: how well does the EuroSCORE predict operative risk for Chinese population? Eur J Cardiothorac Surg. 2009;35(1):54-8. doi:10.1016/j.ejcts.2008.08.001.
5. Ambler G, Omar RZ, Royston P, Kinsman R, Keogh BE, Taylor KM. Generic, simple risk stratification model for heart valve surgery. Circulation. 2005;112(2):224-31. doi:10.1161/CIRCULATIONAHA.104.515049.
6. Florath I, Rosendahl UP, Mortasawi A, Bauer SF, Dalladaku F, Ennker IC, et al. Current determinants of operative mortality in 1400 patients requiring aortic valve replacement. Ann Thorac Surg. 2003;76(1):75-83. doi:10.1016/s0003-4975(03)00341-2. [MedLine]
7. Jin R, Grunkemeier GL, Starr A; Providence Health System Cardiovascular Study Group. Validation and refinement of mortality risk models for heart valve surgery. Ann Thorac Surg. 2005;80(2):471-9. doi:10.1016/j.athoracsur.2005.02.066.
8. Nowicki ER, Birkmeyer NJ, Weintraub RW, Leavitt BJ, Sanders JH, Dacey LJ, et al. Multivariable prediction of in-hospital mortality associated with aortic and mitral valve surgery in Northern New England. Ann Thorac Surg. 2004;77(6):1966-77. doi:10.1016/j.athoracsur.2003.12.035. [MedLine]
9. Kalender M, Baysal AN, Karaca OG, Boyacioglu K, Kayalar N. Validation of German aortic valve score in a multi-surgeon single center. Braz J Cardiovasc Surg. 2017;32(2):77-82. doi:10.21470/1678-9741-2016-0029. [MedLine]
Authors' roles & responsibilities
SCR Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved; final approval of the version to be published
MPBOS Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved; final approval of the version to be published
LRPC Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published
AMP Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; final approval of the version to be published
RGSD Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; final approval of the version to be published
ACEAN Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; final approval of the version to be published
KZ Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; final approval of the version to be published
AR Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; final approval of the version to be published
AW Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; final approval of the version to be published
RCL Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; final approval of the version to be published
Article receive on Friday, September 27, 2019
Article accepted on Wednesday, December 11, 2019
 All scientific articles published at bjcvs.org are licensed under a Creative Commons license
All scientific articles published at bjcvs.org are licensed under a Creative Commons license













All rights reserved 2017 / © 2024 Brazilian Society of Cardiovascular Surgery
DEVELOPMENT BY ![]()

 English PDF
English PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket