![]()
![]()
Walter J. GomesI; Isadora S. RoccoI; Caroline BublitzI; Isis BegotI; Marcela ViceconteI; Walace de Souza PimentelI; Nelson HossneI; Alexandre R. CarvalhoII; Eduardo Gregório ChamlianI; Rita Simone L. MoreiraI; Ross ArenaIV; Solange GuiziliniV
DOI: 10.21470/1678-9741-2019-0289
ABSTRACT
Placement of a mediastinal drain is a routine procedure following heart surgery. Postoperative bed rest is often imposed due to the fear of potential risk of drain displacement and cardiac injury. We developed an encapsulating stitch as a feasible, effective and low-cost technique, which does not require advanced surgical skills for placement. This simple, novel approach compartmentalizes the drain allowing for safe early mobilization following cardiac surgery.CABG = Coronary artery bypass surgery
CR = Cardiac rehabilitation
ICU = Intensive care unit
INTRODUCTION
Mediastinal drain insertion is a routine procedure following cardiac surgery. Although rarely reported, catastrophic complications provoked by mediastinal tubes may occur, such as perforation of cardiac chambers, injuries to the great vessels, damage to coronary grafts, and myocardial ischemia[1,2]. Recently, this issue has drawn renewed attention due to the importance of early postoperative mobilization when the mediastinal tube is still in place.
Early mobilization is an important part of the inpatient cardiac rehabilitation (CR) following surgical heart procedures to improve postoperative recovery (e.g., improves cognitive status and functional capacity). Exercise-based, inpatient CR contributes to a reduced incidence of perioperative complications, decreasing intensive care unit (ICU) and postoperative stay as well as reducing future morbidity and mortality in a cost-effective manner[3].
To ensure that the benefits of early mobilization are achieved while minimizing risk to the patient, we developed a novel operative maneuver; a dedicated stitch aimed to compartmentalize and keep the mediastinal drain insulated from the heart chambers.
TECHNIQUE
This stitch technique was routinely performed on 543 consecutive patients undergoing coronary artery bypass grafting (CABG). In our practice, off-pump CABG comprises >70% of the surgical revascularization procedures. The heart operation is conducted in a usual manner, the pericardium is opened using reversed T incision, alongside the diaphragm. At the completion of the operation, one mediastinal chest tube is inserted behind the sternum through a stab incision in the subxiphoid area. Additionally, pleural drains are placed as needed, coming out through separate incisions in the subxiphoid region. The drains are connected to a vacuum suction system at 15 cmH2O negative pressure.
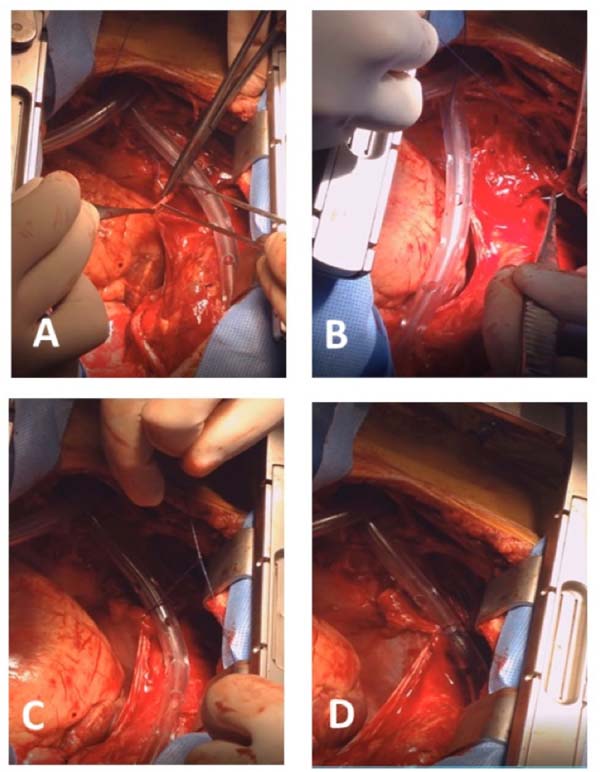
To avoid the mediastinal drain lying directly over the heart, the right aspect of the pericardium is folded around the tube, providing insulation from the heart. To accomplish this, a 4-0 polypropylene stitch is applied to the lower medial edge of the right pericardium (Figure 1A) and sutured to the tissue immediately below the sternum (Figures 1B and 1C), encapsulating the drain and separating it from contact with the heart chambers (Figure 1D); we have named this technique “the safe stitch” (Video 1).

The sternum is closed in a usual manner following drain positioning and confirming stability. All patients were placed in upright position during the first postoperative day before drain removal to evacuate any residual fluid in the pericardial or pleural cavity. The mediastinal tube was removed in a usual manner when the drain flow rate is reduced to approximately zero until the second postoperative day.
DISCUSSION
Contact between the mediastinal drain and heart chambers is a common concern in surgical practice. Beyond the risk of drain displacement and cardiac injury, the vacuum-suction system may stick the drain onto the anterior wall of the right ventricle or to bypass grafts, causing tissue lesions. Although uncommonly described, structural damages could be provoked by drain material in proximity to heart tissue. Complications, such as perforation of the right heart chamber, injuries to coronary grafts or to the great vessels, and myocardial ischemia, have been reported[1,2]. Softer and more flexible drains could help to avoid those lesions. However, it does not solve the issue of contact between drain and heart chambers[4].
Traditionally, in order to reduce the risk of drain displacement, the surgeon and ICU staff are reluctant to place a patient in the upright sitting position for the first hours following surgery. Conversely, early mobilization, a primary component of inpatient CR, has been shown to be effective in reducing postoperative pulmonary complications, reestablishing functional capacity, and decreasing length of ICU stay and postoperative hospitalization days. Studies have shown that early initiation of inpatient CR, including postural changes, during the first postoperative days, is crucial to enhance recovery following cardiac surgery[3,5].
Early removal of mediastinal and pleural drains could be an alternative to reduce one of the hindering factors to early initiation of inpatient CR. However, Andreasen et al.[6] demonstrated that early removal of drains potentially increases the incidence of effusions evolving and the subsequent necessity of further corrective invasive procedures. Therefore, to avoid such postoperative complications, drain removal should respect the proper removal of residual fluid in the pleural or pericardial cavity.
To meet the unique challenges of the cardiac surgery’s postoperative period, allowing for simultaneous preservation of drain placement and early mobilization, we developed the safe stitch to keep the tubular drain away from the heart chambers and the right coronary graft, which is usually close to the mediastinal drain. The drain removal maneuver is harmless and performed as usual. The additional leverage of the safe stitch technique allows for early mobilization strategies with postural changes. Moreover, the safe stitch technique is simple, quickly accomplished, and does not require sophisticated and expensive materials.
The safe stitch technique initiated at our institution has allowed for early mobilization; all patients are placed in an orthostatic sitting position early in the first postoperative day. Later, still in the first postoperative day, an exercise-based CR protocol is initiated, composed of walking and active limb movement.
There has been no incidence of arrhythmias during or immediately after the early initiation of an inpatient CR program in these patients. Bleeding was continuously recorded from the time of sternal closure in the operating room until the drains were removed, usually in the second postoperative day. There was no need for surgical revision due to drain-induced bleeding. No other complications, such as pneumothorax or mediastinal drain displacement, have occurred.
In conclusion, the safe stich technique for drain compartmentalization has allowed for early safe mobilization, initiated early in the first postoperative day, without the occurrence of adverse event related to the mediastinal drain. As such, we recommend that the safe stitch technique should become a routine procedure following open heart surgery.
REFERENCES
1. Uppal RS, O’Keefe PA, Young CP. Perforation of the right ventricleby a suction drain. Cardiovasc Surg 1999;7:261-2.
2. Beiras-Fernandez A, Möhnle P, Kopf C, Vicol C, Kur F, Reichart B. Anuncommon cause of myocardial ischemia after coronary artery bypass grafting:“the dangerous drainage”. Heart Surg Forum 2011;14:E200-1.
3. Neumann FJ, Sousa-Uva M, Ahlsson A, Alfonso F, Banning AP, Benedetto U, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. 2018 Aug 25. doi:10.1093/eurheartj/ehy394.
4. Dantas CE, Sá MP, Bastos ES, Magnanini MM. Pericardium closure after heart operations: a safety option? Rev Bras Cir Cardiovasc 2010;25:365-70. [MedLine]
5. Ramos Dos Santos PM, Aquaroni Ricci N, Aparecida Bordignon Suster É, de Moraes Paisani D, Dias Chiavegato L. Effects of early mobilization in patients after cardiac surgery: a systematic review. Physiotherapy 2017;103:1-12. [MedLine]
6. Andreasen JJ, Sørensen GV, Abrahamsen ER, Hansen-Nord E, Bundgaard K, Bendtsen MD, et al. Early chest tube removal following cardiac surgery is associated with pleural and/or pericardial effusions requiring invasive treatment. Eur J Cardiothorac Surg 2016;49:288-92. [MedLine]
No financial support.
No conflict of interest.
Author's roles & responsibilities
WJG Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved; final approval of the version to be published.
ISR Drafting the work or revising it critically for important intellectual content; final approval of the version to be published.
CB Drafting the work or revising it critically for important intellectual content; final approval of the version to be published.
IB Substantial contributions to the acquisition of data for the work; final approval of the version to be published.
MV Substantial contributions to the acquisition of data for the work; final approval of the version to be published.
WSP Substantial contributions to the acquisition of data for the work; final approval of the version to be published.
NH Substantial contributions to the acquisition of data for the work; final approval of the version to be published.
ARC Substantial contributions to the acquisition of data for the work; final approval of the version to be published.
EGC Substantial contributions to the acquisition of data for the work; final approval of the version to be published.
RSLM Final approval of the version to be published
RA Substantial contributions to the revising it critically for important intellectual content; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved; final approval of the version to be published
SG Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved; final approval of the version to be published
Article receive on Monday, July 15, 2019
Article accepted on Sunday, July 21, 2019
 All scientific articles published at bjcvs.org are licensed under a Creative Commons license
All scientific articles published at bjcvs.org are licensed under a Creative Commons license













All rights reserved 2017 / © 2024 Brazilian Society of Cardiovascular Surgery
DEVELOPMENT BY ![]()


 English PDF
English PDF
 Videos
Videos
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket