![]()
![]()
Taner İyigünI; Mugisha Markior KyaruziI; Barış TimurI; Muhammed Hulusi SatılmışoğluII; Müzeyyen İyigünIII; Mehmet KayaI
DOI: 10.21470/1678-9741-2018-0211
ABSTRACT
Objectives: To investigate the association between clinical hematologic parameters and saphenous vein graft failure after on-pump coronary artery bypass surgery.CAF = Atrial fibrillation
BMI = Body mass index
CABS = Coronary artery bypass surgery
CAD = Coronary artery disease
CAS = Coronary artery surgery
CCTA = Coronary computed tomography angiography
COPD = Chronic obstructive pulmonary disease
CT = Computed tomography
DM = Diabetes mellitus
EF = Ejection fraction
FPG = Fasting plasma glucose
Hb = Hemoglobin
HDL = High-density lipoprotein
LAD-LITA = Left anterior descending-left internal thoracic artery
LD = Low-density lipoprotein
LITA = Left internal thoracic artery
LMCA = Left main coronary artery
MCV = Mean corpuscular volume
MI = Myocardial infarction
MPV = Mean platelet volume
OR = Odds ratio
PCI = Percutaneous coronary intervention
PDW = Platelet distribution width
Plt = Platelet
POAF = Postoperative atrial fibrillation
RDW = Reticulocyte distribution width
ROC = Receiver operating characteristics
SD = Standard deviation
SVG = Saphenous vein graft
WBC = White blood cells
INTRODUCTION
The primary objective of coronary artery bypass surgery (CABS) is to accomplish full revascularization with conduits that will remain patent for the lifetime of the patient. Atherosclerotic factors, such as diabetes mellitus (DM) and older age, can influence graft patency. In addition to these, activities of platelet molecules may play an important role on the initiation and progression of thrombus formation and the inflammatory processes of atherosclerosis[1-3]. Platelet distribution width (PDW) directly measures the variability in platelet size. And larger platelets are both metabolically and enzymatically more active than smaller ones. When there is variation in platelet size (anisocytosis), increased PDW may be evident. Also, platelets with a large size may indicate the presence of platelet aggregates, which may influence the occlusion of a saphenous vein graft (SVG)[4]
The objective of this study was to identify predictive factors for SVG failure in patients undergoing coronary artery surgery (CAS). To do this, all clinical hematological variables were evaluated in the same statistical pool.
METHODS
A total of 1950 consecutive patients underwent CABS in our institute from November 2010 to February 2013. Our study consisted of 284 patients who had undergone coronary computed tomography angiography (CCTA) due to suspicion of progressive coronary artery disease (CAD). Although all patients in our study were under optimal medical treatment, every patient with recurrence of angina symptoms or findings of ischemic changes from noninvasive imaging modalities, such as cardiovascular exercise stress tests or myocardial perfusion scintigraphy, underwent coronary angiography after their surgery.
Of the total 784 distal anastomoses in the patients of our group study, 131 SVG (in 109 patients) were occluded. Sequential and T grafting were used in 13 of 109 patients with at least one graft occlusion. Repeated revascularization was performed in only 13 patients, because their lesions were suitable for treatment with percutaneous coronary intervention.
We reviewed the preoperative and postoperative coronary angiograms of these patients retrospectively. Groups were created according to the presence of at least one SVG failure. In our hospital, patients with stable angina symptoms and/or positive stress test results routinely undergo CCTA examination first. Therefore, conventional coronary angiograms of patients with occluded grafts based on CCTA are elective.
Patients whose SVG were harvested endoscopically, who had previous atrial arrhythmia, infection, inflammatory disease, acute coronary syndrome, severe hepatic diseases, malignant neoplasms, renal failure (serum creatinine level > 2.0 mg/dL), recent history of blood transfusion, hematological disorders such as severe anemia (hemoglobin level < 10 g/dL), concomitant valvular surgery, emergency, and congenital heart disease, without regular follow-up period, and without taking medical treatment consisted of statin or use of beta-blockers after CABS were excluded from the study. Additionally, patients who underwent off-pump surgery or redo surgery were excluded.
Written informed consents were obtained from all patients before enrollment. The study was also approved by the local ethics committee and the institutional review board of the Istanbul Mehmet Akif Ersoy Thoracic and Cardiovascular Surgery Training and Research Hospital (code: 2018-12). The study was consistent with the Declaration of Helsinki.
Surgical Approach
Anesthetic medication, cardiopulmonary bypass, and surgical techniques were similar in all patients. Median full sternotomy was performed in all patients. The left internal thoracic artery was harvested under direct vision. Surgical preparation of the SVG was also performed under direct vision with the aid of a linear incision along the course of the vein using a pair of fine scissors. These veins were not dilated with high pressure prior to grafting. Aortic and unicaval cannulation, standard cardiopulmonary bypass, antegrade intermittent isothermic blood cardioplegia, systemic hypothermia (32°C), and hemodilution were used in all patients. Vein-to-aortic proximal anastomoses were performed using a lateral clamp. All surgeries were performed by the same team of cardiac surgeons and anesthesiologists.
Diagnostic Tools
The CCTA protocol was carried out using dual-source computed tomography with 2 × 128 detector rows = 256 slices (SOMATOM: Definition Flash Siemens Medical Solutions, Forchheim, Germany). All patients underwent the same protocol. All pre-angiographic computed tomographic images were examined to achieve consensus independently by two interventional radiologists on an offline work station (Leonardo; Siemens Medical Solutions, Forchheim, Germany) using a dedicated semiautomatic software program (Volume Viewer, Siemens Medical Solutions, Forchheim, Germany).
Angiographic Approach
Angiography of the native coronary arteries and bypass grafts as well as interventions were carried out by interventional cardiologists with standard methods via femoral or radial access. Injections were performed into both left internal thoracic artery and each vein-to-aorta proximal anastomosis. If the aortic orifice of the vein graft could not be localized, an aortic root injection was performed to localize the graft or its stump. All angiograms were reviewed by two cardiologists and a cardiac surgeon who were independent of this study and blinded to procedural data.
Echocardiographic Assessment
Preoperative transthoracic two-dimensional and doppler echocardiographic assessments were performed using a Vivid S6 with a 3.5 MHz phased array transducer (GE Medical Systems, Horten, Norway). Ejection fraction (EF) values were calculated with the modified Simpson method.
Biochemical Measurements
Hematological parameters were determined within one week before surgery, CCTA, and conventional coronary angiography. Total blood count analyses were obtained using the CELL-DYN Ruby automatic hematology analyzer (Abbott Diagnostics, Aachen, Germany).
Data Collection
All demographic characteristics, laboratory parameters, and clinical characteristics of the patients were obtained by systematic review of the patients’ files and hospital records. The coronary arteries were scored retrospectively using the SYNTAX score system by two cardiologists who were blinded to the categorization and other clinical data. The calculation of the SYNTAX score was based on a previously published method regarding the criteria of the SYNTAX trial (defined as 50% or greater stenosis in any coronary artery with a diameter of 1.5 mm or greater)[5]. Lastly, coronary angiograms of all patients during the preoperative period were used for the score calculation.
Endpoints and Definitions
The primary endpoint was the presence of at least one SVG failure following coronary angiography. We then analyzed predictors for SVG failure by evaluating the clinical hematologic parameters of occluded and non-occluded groups. A graft failure was described as 70% or more stenosis or total occlusion. If a graft had less than 70% stenosis and the whole course of the graft was visualized, it was described as patent. In sequential vein grafts, each segment was analyzed as a separate graft.
Body mass index was calculated using the recorded body weight and height. DM was defined as self-reported physician’s diagnosis or use of antidiabetic medications. Hypertension was defined as blood pressure ≥ 140/90 mmHg and patients under current treatment with antihypertensive medication were accepted as hypertensive. The length of stay was the days spent in the cardiac surgery ward following surgery. A cerebrovascular event was defined as a postoperative central neurological deficit lasting < 72 h with a morphological substrate confirmed by computer tomography imaging that resulted in irreversible brain damage or body impairment. Atrial fibrillation (AF) was defined as absence of a P-wave before each QRS complex and presence of irregular ventricular rate.
Statistical Analysis
All analyses were performed using the software SPSS v22.0 (SPSS Inc., Chicago, IL). Descriptive statistics included mean, standard deviation, median, minimum, maximum, frequency, and ratios. The distribution of the variables was measured by the Kolmogorov-Smirnov test. A Mann-Whitney U test was used for the analysis of quantitative independent data. A chi-square test was used to analyze qualitative independent data and a Fisher’s test was used when the chi-square test conditions were not met. The effectiveness level was investigated by univariate and multivariate logistic regression analyses. Receiver operating characteristics (ROC) analysis was used to calculate the area under the curve for PDW to identify the presence of SVG failure in patients. The ROC curve analysis was performed only for PDW because it was the only predictor among the other hematologic variables per the multiple logistic regression analysis. A conventional ROC curve was generated and the area under the curve was calculated to determine the PDW. The results were evaluated within a 95% confidence interval. All statistical tests were two-sided and significance was determined at P<0.05.
RESULTS
Baseline Characteristics
Two hundred and eighty-four patients (223 men, 61 women) underwent CAS. The mean age was 62 years (range: 31 to 85 years). A total of 109 patients (90 men, 19 women) with mean age of 63.5 years were included in the SVG occluded group and 175 patients (133 men, 42 women) with mean age of 57.6 years were included in the SVG patent group. The rate of SVG failure was not affected by sex (P=0.190). Hematologic parameters and the clinical characteristics of the patients and a comparison of cardiovascular risk factors are summarized in Tables 1 and 2. In the univariate analysis, older age, smoking, EF value, medical history of myocardial infarction (MI), DM, postoperative AF, cerebrovascular events, and preoperative SYNTAX score were statistically significantly different between the two groups. The EF value was lower in the SVG occluded group than in the SVG patent group (P<0.000). When the two groups were compared with respect to laboratory results, serum creatinine level, mean platelet volume, and PDW were statistically significantly higher in patients with occlusion than those without it.
| SVG occluded group | SVG patent group | P value | ||||
|---|---|---|---|---|---|---|
| Mean ± SD/n-% | Mean ± SD/n-% | |||||
| Age (years) | 63.5±7.9 | 57.6±8.5 | 0.000 m | |||
| Sex | Female, n (%) | 19 | 17.4% | 42 | 24% | 0.190 X2 |
| Male, n (%) | 90 | 82.6% | 133 | 76% | ||
| BMI (kg/m2) | 27.9±3.7 | 28.8±4.3 | 0.158 m | |||
| DM, n (%) | 75 | 68.8% | 69 | 39.4% | 0.000 X2 | |
| Hypertension, n (%) | 64 | 58.7% | 88 | 50.3% | 0.166 X2 | |
| Smoking | 71 | 65.1% | 58 | 33.1% | 0.000 X2 | |
| Peripheral arterial disease, n (%) | 8 | 7.3% | 12 | 6.9% | 0.877 X2 | |
| COPD, n (%) | 22 | 20.2% | 28 | 16% | 0.368 X2 | |
| Previous MI, n (%) | 64 | 58.7% | 65 | 37.1% | 0.000 X2 | |
| Previous PCI, n (%) | 42 | 38.5% | 64 | 36.6% | 0.740 X2 | |
| Ejection fraction (%) | 45±8.9 | 56.4±7 | 0.000 m | |||
| Preoperative SYNTAX score | 27.6±9.2 | 23.5±10.1 | 0.000 m | |||

| SVG occluded group | SVG patent group | P value | |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| Total cholesterol level (mg/dL) | 209.2±68.1 | 200±55.2 | 0.404 m |
| HDL (mg/dL) | 38.5±10.5 | 39.4±12.5 | 0.753 m |
| LDL (mg/dL) | 134.7±43.6 | 128.5±45.2 | 0.254 m |
| FPG (mmol/L) | 139.9±62.2 | 136.6±57.8 | 0.867 m |
| HbA1C | 7.2±2.2 | 6.8±1.7 | 0.352 m |
| Hb (gr/dL) | 13.8±1.7 | 13.5±1.6 | 0.232 m |
| MPV (fL) | 8.9±1 | 8.5±1.1 | 0.002 m |
| WBC (x 109/L) | 8.1±1.9 | 7.8±1.9 | 0.290 m |
| Lymphocyte (x 109/L) | 2.3±0.9 | 2.4±0.8 | 0.328 m |
| Neutrophil (x 109/L) | 4.9±1.6 | 4.8±1.5 | 0.712 m |
| MCV (fL) | 86.2±5.9 | 86.2±6.5 | 0.805 m |
| Plt (x1000/mL) | 240.9±78 | 259±87.8 | 0.054 m |
| PDW | 16.9±2 | 15.3±1.2 | 0.000 m |
| RDW | 13.9±1.6 | 13.5±1.3 | 0.056 m |
| Uric acid (mg/dL) | 5.8±1.8 | 5.3±1.4 | 0.269 m |
m Mann-Whitney U Test.
Operative and Postoperative Data
The numbers of bypass grafts and use of red blood cell units in the SVG occluded group were significantly higher than in the SVG patent group (Table 3).
| SVG occluded group | SVG patent group | P value | |||
|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | ||||
| Number of bypass grafts (n) | 3.5±0.8 | 3.1±0.7 | 0.000 m | ||
| Cardiopulmonary bypass time (min) | 108.2±51.3 | 91.2±32.3 | 0.011 m | ||
| Cross-clamp time (min) | 61.6±44.9 | 49.2±23.5 | 0.051 m | ||
| Blood transfusion amount (units) | 4±3 | 2.9±2.2 | 0.001 m | ||
| Follow-up time (months) | 49.96±3.93 | 48.89±4.06 | 0.072 m | ||
| Interval from operation to CT angiogram (months) | 40.0±3.9 | 39±3.6 | 0.242 m | ||
| LAD-LITA | 108 | 99.1% | 170 | 97.1% | 0.269 X2 |
| Occluded LITA | 4 | 3.7% | 3 | 1.7% | 0.301 X2 |
| LMCA | 17 | 15.6% | 21 | 12% | 0.387 X2 |
| Clopidogrel | 15 | 13.8% | 12 | 6.9% | 0.054 X2 |
| Sequential anastomosis | 9 | 8.3% | 8 | 4.6% | 0.203 X2 |
| T graft | 4 | 3.7% | 1 | 0.6% | 0.073 X2 |
| POAF | 31 | 28.4% | 32 | 18.3% | 0.045 X2 |
| Cerebrovascular incident, n (%) | 7 | 6.4% | 2 | 1.1% | 0.013 X2 |
| Length of stay in hospital (days) | 9.6±6.3 | 8.5±2.9 | 0.223 m | ||

Cumulative Analysis
In a multivariate logistic regression model, a significant association was found between graft occlusion and older age, DM, PDW, history of previous MI, and EF (Table 4).
| Univariable model | Multivariable model | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% confidence interval | P | OR | 95% confidence interval | P | |||||
| Age | 1.10 | 1.06 | - | 1.13 | 0.000 | |||||
| Blood transfusion amount | 1.19 | 1.08 | - | 1.31 | 0.000 | |||||
| Smoking | 3.77 | 2.28 | - | 6.24 | 0.000 | 3.17 | 1.14 | - | 8.81 | 0.027 |
| Diabetes mellitus | 3.39 | 2.04 | - | 5.62 | 0.000 | 3.46 | 1.21 | - | 9.83 | 0.020 |
| Prevıous MI | 2.41 | 1.48 | - | 3.93 | 0.000 | |||||
| POAF | 1.78 | 1.01 | - | 3.13 | 0.047 | |||||
| Cerebrovascular incident | 6.00 | 1.22 | - | 29.41 | 0.027 | |||||
| MPV | 1.42 | 1.13 | - | 1.80 | 0.003 | |||||
| PDW | 2.38 | 1.73 | - | 3.27 | 0.000 | 3.53 | 1.97 | - | 6.35 | 0.000 |
| Ejection fraction | 0.85 | 0.82 | - | 0.88 | 0.000 | 0.84 | 0.79 | - | 0.89 | 0.000 |
| Creatinine | 72.2 | 20.5 | - | 255.1 | 0.000 | |||||
| Cardiopulmonary bypass time | 1.01 | 1 | - | 1.02 | 0.009 | |||||
| Preoperative SYNTAX Score | 1.04 | 1.02 | - | 1.07 | 0.001 | 1.07 | 1.01 | - | 1.13 | 0.013 |
| Number of grafts | 1.82 | 1.32 | - | 2.50 | 0.000 | |||||

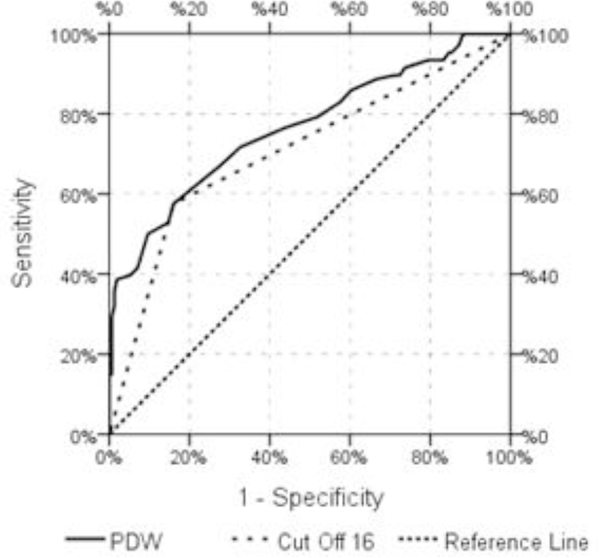
Receiver Operator Characteristic Curve Analysis
The area under the ROC curve (95% confidence interval) for PDW as a predictor of SVG failure was 0.765 (0.70-0.82, P<0.000) (Figures 1 and 2). The PDW cut-off point was > 16 for a sensitivity of 57.5% and specificity of 84%.
DISCUSSION
In this study, we investigated the relationship between SVG failure and the clinical hematological parameters of patients who had undergone CABS. We found that age, DM, history of previous MI, and PDW were significantly associated with vein graft failure. A history of previous MI and protected left ventricular functions yields similar results. In other words, MI can cause decreased ventricular function. Apart from these factors, our study demonstrated that a good EF was a protective factor against SVG failure. Older age and DM can be thought of as preoperative and non-specific factors. Therefore, it is difficult to estimate post-operative SVG failure. However, PDW is both a specific and pre-angiographic predictive parameter for SVG failure after the procedure and PDW is a more specific marker of platelet activation than other platelet indices, such as mean platelet volume, because PDW does not increase during simple platelet swelling[6]. For these reasons, PDW may provide valuable predictive information regarding the potential for SVG failure following CABS.
The occlusion or stenosis of SVG within the first year after the operation is attributed to surgical technical errors, thrombosis, and occlusive intimal hyperplasia[7]. Beyond one year, inflammation that causes increased platelet activation plays a major role in the development of atherosclerosis[2]. Platelet count, mean platelet volume, and PDW may reflect the degree of platelet activation. The relationship between atherosclerosis and increments in platelet activity is well known.
However, there is not a great deal of data regarding the relationship between PDW and SVG failure. Moreover, contrasting results have been reported[8]. It is clear that all aspects of this issue need to be deeply considered. A very limited number of studies have been performed examining the pathophysiology between PDW and SVG failure since the first description of this relationship by Ege et al.[2], in 2013. Regarding our study results, platelet activators, such as increased PDW, may initiate or accelerate atherosclerosis. Therefore, it is important to slow down platelet activation and inflammation. Additionally, PDW may not be the only parameter associated with atherosclerotic processes, but the red blood cell distribution width may also play an important role[9]. The inflammation that is involved in arterial atherosclerosis might contribute to an increased red blood cell distribution[10]. Although this distribution was not statistically significantly different between the two groups, it approached statistical significance. It can be seen as a subtle contribution.
DM is a well-known cardiovascular risk factor; graft stenosis is more frequent in diabetic patients compared with patients with other risk factors. Surgical treatment is considered to be the standard method for diabetic patients with advanced multivessel diseases[11]. In addition to this, DM may induce a ‘prothrombotic state’ with enhanced platelet reactivity. Jindal et al[12]. observed that there is a significant association between PDW and microvascular dysfunction in patients with DM.
Reduced EF was observed in this study to be independently correlated with the rate of vein graft patency, as observed in other studies[13,14]. This may happen as a result of the need of high coronary blood flow for large myocardial ischemic areas. A normal EF may also indicate ischemic myocardium with a sufficient distal runoff.
An increased time interval after CABS is linked to atherosclerosis of the grafts. Doğan et al.[15] reported that the age of the SVG is useful for prediction of SVG failure, with the risk increasing over time. We observed similar results in the follow-up of the patients in this study.
The complexity of coronary artery atherosclerosis is determined using the SYNTAX score system. Its validity is well known and well codified[5]. Considering this information, we found reduced graft patency in patients with high SYNTAX scores. In this context, the SYNTAX score can be seen as a strong predictive factor according to our multivariable model. Atherosclerosis is an ongoing disease process throughout the arterial system[16]. Correspondingly, patients with CAD may have extensive atherosclerosis in other arterial branches, such as the carotid artery. As a result, these patients may experience adverse events, such as cerebrovascular events, due to the progressive nature of the atherosclerosis. In fact, the rate of transient ischemic attack and/or stroke was higher in patients in the SVG occluded group than in the SVG patent group during the post-surgical period.
The duration of the cardiopulmonary bypass, serum creatinine levels, and mean platelet values are other risk factors for progression of atherosclerosis in the coronary artery in the remote future following coronary artery bypass grafting. However, these factors did not have a significant influence in the multivariable analyses in our study.
Limitations
This study has some inherent limitations by virtue of being retrospective. Only routine laboratory parameters were measured in this study; therefore, other mediators were not examined. Another issue is that this was a single-center study, so our results need to be confirmed and supported by a larger sample of patients than we reported. Another limitation of this study is that patients had elective angiography for a variety of reasons. Our findings also do not include patients’ outcomes such as acute coronary syndrome or death during the post-operative period. Finally, the analysis of graft patency is less accurate with CCTA than with conventional coronary angiography. Even though dual-source computed tomography scanning with 2 × 128 detector rows covers the whole heart in a short period of time, improper timing of the scan can generate a false-negative evaluation. This may be a drawback in terms of graft assessment.
CONCLUSION
In conclusion, older age and DM are associated with SVG failure. In addition to these, increased PDW can indicate progression to SVG failure and platelet activation might accelerate disease in the veins, leading to closure. Our results are clinically significant because increased PDW is easily measured and can be used as a simple and valuable marker for prediction of SVG failure.
REFERENCES
1. Parang P, Arora R. Coronary vein graft disease: pathogenesis andprevention. Can J Cardiol. 2009;25(2):e57-e62.doi:10.1016/S0828-282X(09)70486-6.
2. Ege MR, Guray U, Guray Y, Acikgoz S, Demirkan B. Plateletdistribution width and saphenous vein disease in patients after CABG.Association with graft occlusion. Herz. 2013;38(2):197-201.doi:10.1007/s00059-012-3668-z. [MedLine]
3. Fuentes QE, Fuentes QF, Andrés V, Pello OM, Font de Mora J, PalomoGI. Role of platelets as mediators that link inflammation and thrombosis inatherosclerosis. Platelets. 2013;24(4):255-62.doi:10.3109/09537104.2012.690113.
4. Rechcinski T, Jasinska A, Forys J, et al. Prognostic value ofplatelet indices after acute myocardial infarction treated with primarypercutaneous coronary intervention. Cardiol J. 2013;20(5):491-8.doi:10.5603/CJ.2013.0134.
5. Serruys PW, Morice MC, Kappetein AP, et al. Percutaneous coronaryintervention versus coronary-artery bypass grafting for severe coronary arterydisease. N Engl J Med. 2009;360(10):961-72.doi:10.1056/NEJMoa0804626.
6. Vagdatli E, Gounari E, Lazaridou E, Katsibourlia E, Tsikopoulou F,Labrianou I. Platelet distribution width: a simple, practical and specificmarker of activation of coagulation. Hippokratia . 2010 ;14(1):28-32. Available from:
7. Sabik JF 3rd. Understanding saphenous vein graft patency.Circulation. 2011;124(3):273-5.doi:10.1161/CIRCULATIONAHA.111.039842.
8. De Luca G, Venegoni L, Iorio S, et al. Platelet distribution widthand the extent of coronary artery disease: results from a large prospectivestudy. Platelets. 2010;21(7):508-14.doi:10.3109/09537104.2010.494743.
9. Akyel A, Celik IE, Oksüz F, et al. Red blood cell distribution widthin saphenous vein graft disease. Can J Cardiol. 2013;29(4):448-51.doi:10.1016/j.cjca.2012.06.015.
10. Wen Y. High red blood cell distribution width is closely associatedwith risk of carotid artery atherosclerosis in patients with hypertension. ExpClin Cardiol . 2010 ;15(3):37-40. Available from:
11. Farkouh ME, Domanski M, Sleeper LA, et al. Strategies formultivessel revascularization in patients with diabetes. N Engl J Med.2012;367(25):2375-84. doi:10.1056/NEJMoa1211585.
12. Jindal S, Gupta S, Gupta R, et al. Platelet indices in diabetesmellitus: indicators of diabetic microvascular complications. Hematology.2011;16(2):86-9. doi:10.1179/102453311X12902908412110.
13. Korpilahti K, Engblom E, Syvänne M, et al. Angiographic changes insaphenous vein grafts and atherosclerosis risk factors. A 5-year study withserial measurements of serum lipids and lipoproteins. Scand Cardiovasc J.1998;32(6):343-51. doi:10.1080/14017439850139799.
14. Nakajima H, Iguchi A, Tabata M, et al. Predictors and prevention of flow insufficiency due to limited flow demand. J Cardiothorac Surg. 2014:9:188. doi:10.1186/s13019-014-0188-3. [MedLine]
15. Dogan M, Akyel A, Cimen T, et al. Relationship between neutrophil-to-lymphocyte ratio and saphenous vein graft disease in patients with coronary bypass. Clin Appl Thromb Hemost. 2015;21(1):25-9. doi:10.1177/1076029613488935. [MedLine]
16. Ahmadi A, Leipsic J, Blankstein R, et al. Do plaques rapidly progress prior to myocardial infarction? The interplay between plaque vulnerability and progression. Circ Res. 2015;117(1):99-104. doi:10.1161/CIRCRESAHA.117.305637. [MedLine]
No financial support.
No conflict of interest.
Authors' roles & responsibilities
TI Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; final approval of the version to be published
MMK Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; final approval of the version to be published
BT Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; final approval of the version to be published
MHS Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; final approval of the version to be published
MI Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; final approval of the version to be published
MK Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; final approval of the version to be published
Article receive on Sunday, July 22, 2018
Article accepted on Monday, December 17, 2018
 All scientific articles published at bjcvs.org are licensed under a Creative Commons license
All scientific articles published at bjcvs.org are licensed under a Creative Commons license













All rights reserved 2017 / © 2024 Brazilian Society of Cardiovascular Surgery
DEVELOPMENT BY ![]()


 English PDF
English PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket