![]()
![]()
João Roberto Breda; Gustavo Calado de Aguiar Ribeiro
DOI: 10.5935/1678-9741.20110021
ABSTRACT
When atrial fibrillation (AF) is present in pre-operative open heart surgeries, including coronary artery bypass grafting and valve operations, it represents an independent risk factor for cardiac events and reduced survival. Due to the complexity of the subject, especially when evaluating success rates (reversion and maintenance of normal sinus rhythm), a consensus statement was recently proposed by the International Society of Minimally Invasive Cardiothoracic Surgery (ISMICS), in order to determine whether the intraoperative ablation of AF promotes favorable clinical outcomes in patients undergoing other cardiac operations in comparison with individual operations without ablation. The aim of this paper is to present published data which has contributed to consensus statement and can be useful as update source. The integrative review was the methodology that provides synthesis of knowledge and applicability of results of significant studies about presented topicRESUMO
A fibrilação atrial (FA) no pré-operatório de operações cardíacas abertas, incluindo revascularização cirúrgica do miocárdio (RCM) e operações valvares, representa fator de risco independente para eventos cardíacos maiores e redução de sobrevida. Devido à complexidade do assunto, principalmente na avaliação das taxas de sucesso, foi proposta recentemente uma declaração de consenso pela International Society of Minimally Invasive Cardiothoracic Surgery (ISMICS), com o intuito de determinar se a ablação operatória da FA promove resultados clínicos favoráveis em pacientes submetidos a outras operações cardíacas na comparação com operações isoladas sem ablação. O objetivo deste trabalho é apresentar dados da literatura que possam contribuir para o consenso sobre o tratamento operatório da FA e ser utilizado como fonte de atualização. A metodologia envolveu revisão integrativa da literatura, com análise e síntese dos dados obtidos de forma descritiva, apresentando o conhecimento atual sobre o tema apresentadoINTRODUCTION
Atrial fibrillation (AF) in the preoperative of open heart surgery, including coronary artery bypass grafting (CABG) and valve operations, represents an independent risk factor for major cardiac events and reduced survival [1-3].
The result of surgical ablation of AF remains controversial, although randomized prospective studies have shown significant differences in return to sinus rhythm in patients treated with ablation vs control group, however, further studies are needed to confirm the impact on clinical outcomes and quality of life of these patients [4-6].
So with the growing interest in understanding the pathophysiology responsible for the occurrence of this arrhythmia, surgical techniques have been developed in order to increase the effectiveness of this operation and reduction of the possibility of treatment failure, which can reach 20% of patients undergoing treatment arrhythmia in association with mitral valve surgery [7,8]. The main factors involved in the failure of the procedure are left atrial diameter, age, long-term AF, permanent AF, incomplete ablation lines with uniatrial approach and non-transmural lesion [9-11].
In 2007, joint publication of the Heart Rhythm Society and Society of Thoracic Surgeons (STS) concluded that the indications for surgical treatment of AF are: symptomatic AF in patients undergoing other cardiac procedures, asymptomatic AF only in selected patients, AF alone in symptomatic patients who opted for surgical treatment after one or more attempts at catheter ablation without success [5]. Despite the great importance of this publication in an attempt to standardize the indications of surgical treatment of AF, due to the complexity of the subject mainly to evaluate the success rates, it has been recently proposed a consensus statement by the International Society of Minimally Invasive Cardiothoracic Surgery (ISMICS) in order to determine whether the surgical ablation of atrial fibrillation promotes favorable clinical outcomes in patients undergoing other cardiac operations, particularly the valve repair and/or coronary artery bypass grafting (CABG), compared to a single transaction without ablation [12].
The aim of this study is to present data in the literature, which may contribute to the consensus on the surgical treatment of AF and be used as an update source.
METHODS
Integrative review to search for articles in the following databases: the Latin American and Caribbean Health Sciences (LILACS) and Medical Literature Analysis and Retrieval System Online (MEDLINE). We included articles published in Portuguese and English, related to the topic presented, published in these databases in the last 15 years. The keywords of the research were: atrial fibrillation, ablation techniques and results of treatment.
The analysis and synthesis of data were performed in a descriptive way, in order to present the current knowledge about the surgical treatment of AF [13].
Thus, after identification of the subject (surgical treatment of atrial fibrillation) it was defined the research question: In patients with AF at the time of other cardiac operations, is intraoperative ablation of tachyarrhythmia able to restore and maintain sinus rhythm with a potential improvement of the results compared to cardiac operations without ablation?
We included randomized and nonrandomized studies (with acceptable designs approaching the proposed topic), experimental studies to fully understand the phenomenon and other data with the theoretical literature.
Studies approaching catheter ablation and surgical treatment of lone AF were excluded from this study.
RESULTS
The literature review resulted in 48 articles, which were divided according to type of publication and sampling: two randomized trials (368 patients), 20 non-randomized studies (3788 patients), 12 experience reports, seven literature reviews, four experimental and three consensus statements.
The studies were analyzed and summarized taking into account the sample, methodology, results and conclusions.
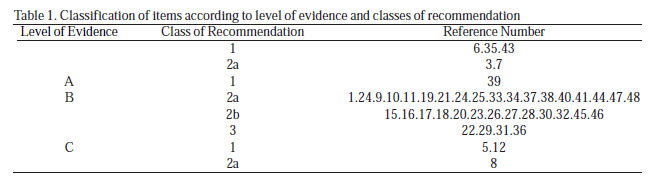
The best evidences available were classified according to the recommendations proposed by the American Heart Association (AHA)/American College of Cardiology (ACC), defined as follows: LEVELS OF EVIDENCE - A (data from multiple randomized clinical trials), B (data derived from single randomized trials or nonrandomized studies) and C (expert opinion); CLASS OF RECOMMENDATION - 1 (conditions where there is evidence and/or general agreement that the procedure or treatment is useful and effective), 2 (conditions where there is conflict and/or dissenting opinion about the usefulness/effectiveness of the procedure or treatment. The evidences were subdivided into 2a- when the opinion is in favor of usefulness/effectiveness and 2b, when the usefulness/efficacy is less established by the opinion) and 3 (conditions where there evidence and/or general agreement that the procedure/treatment is not useful or effective and in some cases may be harmful).
Given this classification, the study has been defined and the results are presented in Table 1.
DISCUSSION
Ablation of atrial tissue
Ablation of atrial tissue can be obtained in several ways besides the traditional technique of cut and suture, the major alternative energy sources developed for this purpose are: cryoablation, radiofrequency, microwave, high intensity ultrasound and laser. In the following paragraphs we briefly describe these sources of energy and results in the literature.
Cryoablation
Currently, there are two sources of criotermal energy commercially available, one that uses nitric oxide and other argon, the difference between the two is the ability to freeze the tissue. Nitric oxide is capable of producing temperatures of -89.5ºC and argon can achieve -185.7ºC, both in terms of atmosphere (1 atm) pressure. The size and depth of the lesion will depend on several factors: temperature catheter cryoablation, tissue temperature, size of catheter, duration and amount of ablation lines, and particularly the cooling agent used (nitric oxide applied for 2 to 3 minutes in the endocardium was effective in generating transmural lesions, as with the use of argon there are insufficient data to evaluate the dose-effect ideal to obtain effective response) [14-16].
Cryoablation has the great advantage of preserving tissue architecture of the heart (with the exception of the coronary arteries) and represents a technology with proven efficacy and safety. The potential disadvantage involves the long duration of application of this energy source (1 to 3 minutes). Moreover, its use is limited in minimally invasive technique because, with the heart beating, freezing can lead to blood clotting and increased risk of thromboembolic events [14].
In 2007, Blomström-Lundqvist et al. [6] published a prospective, multicenter, randomized study to evaluate the effectiveness of cryoablation applied to the epicardium of the left atrium in patients undergoing mitral valve surgery. They analyzed 69 patients who underwent valve surgery alone and in combination with cryoablation. During follow-up, heart rate was set at 6 and 12 months, the rate of sinus rhythm in patients undergoing ablation was 73.3% (in both periods) and without ablation group was 45.7% (6 months ) and 42.9% (12 months) with a significant difference between the two groups in follow-up periods. The authors concluded for the benefit of cryoablation in the reversion and maintenance of sinus rhythm in patients undergoing mitral valve surgery [6].
Radio frequency
The radiofrequency initially used in the electrophysiology laboratory was the first alternative energy source applied in the surgical treatment of AF and has been extensively tested in recent years and may be uni-or bipolar [17].
The irrigated unipolar device produces linear lesion tissue, applying the power source "point to point". The bipolar catheter is able to promote an ablation of all tissue involved by the electrodes and quickly (usually less than 10 seconds). The conduct of energy can be measured during ablation and this may be correlated with proven transmural lesion [18,19]. In experimental studies, obtaining transmural unipolar radiofrequency application requires extended time (over two minutes) and noted that during mitral valve surgery after two minutes of endocardial unipolar ablation, only 20% of lesions were transmural [20]. On the other hand, the bipolar radiofrequency in animal and human studies, was able to produce transmural lesions with a mean ablation of 50 to 10 seconds [21]. Possible complications of the device is unipolar myocardial infarction due to the involvement of coronary arteries, stroke, and esophageal perforation, events that are not related to the biatrial application [22].
Thus, irrigated RF as an energy source alternative to surgical ablation of AF has recognized effectiveness, with success rate of reversion to sinus rhythm that may vary between 75 and 80% [11,23,24]. In 2008, Beukema et al. [25] reported medium and long-term follow-up after radiofrequency ablation associated with other cardiac surgery and demonstrated maintenance of sinus rhythm in 69% of patients treated at 1 year follow-up, 56% in 3 years, 52% in 5 years , and 57% in later periods. Antiarrhythmic drug therapy was maintained in 64% of surviving patients who were free from AF and only 1% were under oral anticoagulation.
Microwave
The energy uses microwave heating by an electromagnetic field generated by the oscillation of molecules from the tissue, producing heat and local ablation with uniform penetration without burn the surrounding tissues [26]. This source of energy seems to produce transmural lesions after 90 seconds of application, in an experimental model with heart stopped, but in models with beating heart, there is controversy regarding the transmurality of lesions produced, which could limit the application of minimally invasive operations [27,28]. Due to the heat generated by the device during the ablation, there are reports of complications in coronary artery susceptible to stenosis and also concern about possible perforation of the esophagus. Publication with 600 patients operated with this device reported no major complications, confirming its safety and efficacy as well (with reversion to sinus rhythm between 70 and 90% of treated cases) [29,30].
In 2008, Vicol et al. [31] reported long-term monitoring of 41 patients who underwent endocardial ablation for microwave treatment of permanent AF, after 5 years of follow-up, only 39.3% of patients were in sinus rhythm, concluding that the method is not reliable maintenance of sinus rhythm in the long-term.
Laser
Ablation produced by laser beams can be narrow and deep with a short time of application, thus representing an attractive energy source for treatment of AF. However, their ability to create transmural lesions still requires confirmation, especially in clinical applications where the data are still insufficient to detect the effectiveness of the method [32].
This form of energy in addition to be promise has only been tested in experimental studies, with satisfactory results in terms of efficacy and safety [33]. The group from Columbia University in New York used the laser in eight patients underwent surgical treatment of AF and after 1 year of follow-up, six (75%) were in sinus rhythm, the authors suggest that this new technology may offer advantages over other existing methods, with possible reduction of side effects [34].
High-intensity ultrasound
The use of ultrasound to treat AF by involves tissue damage by hyperthermia with necrosis of the tissue and can be used in order to focus the waves of high intensity, capable of producing transmural lesions after 2 seconds of application [35]. The use of this technology has attracted interest because it allows ablation non-invasively and without contact with the focal tissue, decreasing the chance of affecting surrounding structures [36,37].
In Brazil, Brick et al. [38] published the results of 27 patients undergoing the application of ultrasound for treatment of AF and had reversion to sinus rhythm in 81.4% of cases at hospital discharge. The use of epicardial ultrasound was evaluated in patients with ischemic disease, and in at least 6 months of follow-up, we observed a success rate of 85% of patients free from tachyarrhythmias (atrial flutter or atrial fibrillation) [39].
Importance of injury pattern
In 1998, Haïssaguerre et al. [40] published the first time that most episodes of AF is induced by focal triggers localized around the orifices of the pulmonary veins, this allowed the incorporation of multiple surgical energy sources developed primarily for ablation around the pulmonary veins. The introduction of these two changes in the surgical treatment of atrial fibrillation (new energy sources and types of injury) led to confusion in interpreting the possible therapeutic failures of this technique. Although studies suggest that the source of energy used is directly implicated in the favorable outcome of therapy, the importance of the injury pattern in the efficacy of treatment is still essential to the successful outcome [41,42].
The main goal of most surgical treatment of AF has been the possibility of performing this procedure in a less invasive manner, and on this premise, the type of injury is relegated to a secondary, although obtaining the best result should be based in two key concepts: the pattern of injury ablation should be consistent (independent of the access via and the source of energy used) and must involve both atria [43]. Barnett & Ad [44] published an extensive meta-analysis involving 69 studies and 5885 patients, demonstrating that the best results are obtained with contiguous and transmural lesions applied biatrially.
This study reinforces the concept that the operation history of the classic "cut and suture" is more effective not only because the incisions are contiguous and transmural, but mainly by the correct standard of application in terms of location. In summary, all sources of energy should have the same success rate than the classical operation of "cut and suture", since in addition to transmural ablation the lines were applied in the correct locations [43].
In most cases, therapeutic failure is attributed to the power supply and there is no pattern of injury, this may cause a mistake in interpreting the results, preventing the development of promising alternative energy sources for AF ablation (case of laser and microwave). In a recent study, Cox [43] comments that the failure of AF ablation is associated with changes in the Maze' operation (Maze III), involving only the pulmonary vein isolation and left atrial appendage closure.
Thus, the so-called Wolf Mini-Maze performs the isolation of pulmonary veins in a minimally invasive manner, but offers no advantages over catheter ablation [45]. Another modification called Ex-Maze procedure uses radio frequency as an energy source and, despite the injuries showed a similar pattern of classical operation, it fails to treat the atrium as the technique does not include lines in the mitral annulus, coronary sinus and atrium right. Although, it should be highlighted the innovative character of this modification that would allow the endoscopic treatment of atrial fibrillation with epicardial ablation alone [46]. Recently, Edgerton et al. [47] published a study with a pattern of "electrophysiologically" injury equivalent to the classical lesions of the Cox Maze III operation, a procedure called "Dallas lesion set". This concept was considered incorrect in the Cox Review, because it is part of the application of technical line in the right atrium and the pattern of injury would be ineffective in the prevention of atypical left atrial flutter. In addition, the Dallas technique suggests that the proposed standard could allow transmural lesions with any of the sources of energy currently available, be applied in an epicardial manner and under beating-heart, statements that require subsequent confirmation [43].
The development of minimally invasive operations with greater application of epicardial lines, in combination with standard lesions without complete confirmation of effectiveness, may lead to confusion in cases of failure, it remains doubtful whether treatment failure is associated with power supply or standard injury.
ISMICS Consensus - International Society of Minimally Invasive Cardiothoracic Surgery (2009)
The aim of this consensus statement was to determine whether surgical ablation of AF during concomitant cardiac procedures improves clinical outcomes after surgery. The group involved in the study analyzed the best available evidence, a systematic review of data, including randomized trials, controlled or not, always in order of decreasing importance. A systematic review and meta-analysis identified 10 randomized trials (650 patients) and 23 non-randomized trials (3997 patients), most were published in English and performed in the United States [12].
The results obtained are summarized as follows in terms of level of evidence and grades of recommendation:
1. Surgical ablation of AF improves the chance of re-establishing sinus rhythm at discharge and at 1 year follow-up (level), this effect is maintained at 5 years (level B). It does not reduce the use of antiarrhythmic drugs in 12 months after surgery (level), despite the studies were not designed to answer this question;
2. The operation does not increase the need for permanent pacemaker implant (level);
3. It does not increase operative mortality (level A), stroke (CVA) (level A), myocardial infarction (level B), cardiac tamponade (level A), reoperation for bleeding (level A), esophageal perforation (level B) , low cardiac output syndrome (level A), use of intra-aortic balloon (level B), congestive heart failure (CHF) (level B), pleural effusion (level A), pneumonia (level A), renal dysfunction (level B) and mediastinitis (level);
4. It does not reduce mortality at 1 year (level). There is a possible reduction in mortality after one year (level B), but no difference in the incidence of stroke (level A), myocardial infarction (level A) and CHF (B level);
5. There was an increase in exercise tolerance at 1 year (level), but no favorable impact on quality of life at 3 months and 1 year (level), but the methodology and the number of studies is considered insufficient for determination;
6. The increase in the time of anoxia and perfusion produces no difference in length of stay in intensive care unit and hospital stay (grade A).
The authors of the consensus identified as limitations of the study that could weaken the conclusions, the following factors:
• the study had endpoints not uniform and different definitions of success and failure of treatment;
• Insufficient description of the technical modifications employed in terms of type of injury and the energy source;
• monitoring and surveillance of cardiac rhythm very heterogeneous;
• over 1 year of follow-up incomplete, especially in nonrandomized studies;
• lack of discussion of the importance and influence of left atrial diameter in the results;
• special subgroups (age and low ejection fraction) have not been sufficiently studied;
• use of oral anticoagulation after the procedure without a defined protocol;
• consensus did not include the participation of electrophysiologists.
Thus, after these considerations and review of the best available evidence, the authors defined the following consensus recommendations: In patients with persistent and permanent AF, ablation surgery is recommended to increase the incidence of sinus rhythm in the short and long-term (class 1, Level A) to reduce the risk of stroke and thromboembolic events (second class, level A), increase exercise tolerance and improve ventricular function (second class, level A) and increase survival (second class, level B).
FINAL CONSIDERATIONS
The aim of surgical ablation techniques of atrial fibrillation is to keep the patient free of arrhythmia. This concept should have the same meaning for all researchers of this subject, but still controversial. Thus, after follow-up period from 3 to 6 months, all cases of recurrence of AF, atrial flutter and right atypical left atrial flutter should be considered treatment failure [43]. Clinically, patients tolerate better AF than atrial flutter if after ablation surgery successfully performed the pace is no longer of AF and becomes atrial flutter; some authors consider as success of the technique, what produces a mistaken interpretation of the results and accuracy of the method [48].
Today, the notion that success rates of surgical ablation of atrial fibrillation between 70 and 80% of cases is satisfactory may not be more valid, since in that recent upgrade to 16,309 patients undergoing treatment in the electrophysiology laboratory showed similar results [ 49].
Thus, some concepts need to be observed when making a decision on the surgical treatment of AF, if the operation requires opening the left atrium, the mitral annulus should be involved in the ablation; if involving right atriotomy, the option should be for biatrial ablation; in presence of long-term symptomatic AF, the result is also better with the biatrial technique, in CABG or aortic valve replacement with AF of short duration, considering the isolation of pulmonary veins and finally, when the subject is an indication of tachyarrhythmia or if it is desired best results, the classical operation of "cut and suture" should be the method of choice.
Many authors agree that the future of this operation will depend on the possibility of performing a minimally invasive procedure (endoscopic or robotic), avoiding general anesthesia, endotracheal intubation and chest tubes. In addition, surgeons should be alert to obtain satisfactory results above the current 80% and mainly to provide an effective and definitive treatment to the patient with this arrhythmia.
REFERENCES
1. Ngaage DL, Schaff HV, Mullany CJ, Sundt 3rd TM, Dearani JA, Barnes S Does preoperative atrial fibrillation influence early and late outcomes of coronary artery bypass grafting. J Thorac Cardiovasc Surg. 2007;133(1):182-9. [MedLine]
2. Ngaage DL, Schaff HV, Mullany CJ, Barnes S, Dearani JA, Daly RC Influence of preoperative atrial fibrillation on late results of mitral valve repair : is concomitant ablation justified?. Ann Thorac Surg. 2007;84(2):434-42.
3. Lim E, Barlow CW, Hosseinpour AR, Wisbey C, Wilson K, Pidgeon W Influence of atrial fibrillation on outcome following mitral valve repair. Circulation. 2001;104(12):I59-63. [MedLine]
4. Kalman J, Munuwar M, Howes LG, Louis WJ, Buxton BF, Gutteridge G Atrial fibrilation after coronary artery bypass grafting is associated with sympathetic activation. Ann Thorac Surg. 1995;60(6):1709-15. [MedLine]
5. Calkins H, Brugada J, Packer DL, Cappato R, Chen SA, Crijins HJ HRS/EHRA/ECAS expert Consensus Statement on catheter and surgical ablation of atrial fibrillation : recommendations for personnel, policy, procedures and follow-up. A report of the Heart Rhythm Society (HRS) Task Force on catheter and surgical ablation of atrial fibrillation. Heart Rhythm. 2007;4(6):816-61. [MedLine]
6. Blomström-Lundqvist C, Johansson B, Berglin E, Nilsson L, Jensen SM, Thelin S A randomized double-blind study of epicardial left atrial cryoablation for permanent atrial fibrillation in patients undergoing mitral valve surgery : the SWEDish Multicentre Atrial Fibrillation study (SWEDMAF). Eur Heart J. 2007;28(23):2902-8. [MedLine]
7. McCarthy PM, Kruse J, Shalli S, Ilkhanoff L, Goldberger JJ, Kadish AH Where does atrial fibrillation surgery fail : Implications for increasing effectiveness of ablation. J Thorac Cardiovasc Surg. 2010;139(4):860-7. [MedLine]
8. Shemin RJ, Cox JL, Gillinov AM, Blackstone EH, Bridges CR Guidelines for reporting data and outcomes for the surgical treatment of atrial fibrillation. Ann Thorac Surg. 2007;83(3):1225-30. [MedLine]
9. Gillinov AM, Bhavani S, Blackstone EH, Rajeswaran J, Svensson LG, Navia JL Surgery for permanent atrial fibrillation : impact of patient factors and lesions set. Ann Thorac Surg. 2006;82(2):502-13.
10. Gillinov AM, Bakaeen F, McCarthy PM, Blackstone EH, Rajeswaran J, Petterson G Surgery for paroxysmal atrial fibrillation in the setting of mitral valve disease : a role for pulmonary vein isolation?. Ann Thorac Surg. 2006;81(1):19-26. [MedLine]
11. Breda JR, Ragognette RG, Breda ASCR, Gurian DB, Horiuti L, Machado LN Avaliação inicial da ablação operatória biatrial por radiofrequência de fibrilação atrial. Rev Bras Cir Cardiovasc. 2010;25(1):45-50. [MedLine] View article
12. Ad N, Cheng DCH, Martin J, Berglin EE, Chang BC, Doukas G Surgical Ablation for atrial fibrillation in cardiac surgery : a consensus statement of the International Society of Minimally Invasive Cardiothoracic Surgery (ISMICS) 2009. Innovations. 2010;5(2):74-83.
13. Souza MT, Silva MD, Carvalho R Revisão integrativa : o que é e como fazer. Einstein. 2010;8:102-6.
14. Voeller RKI, Schuessler RB, Damiano R, Cohn LH Surgical treatment of atrial fibrillation2008;:1375-94.
15. Lustgarten DL, Keane D, Ruskin J Cryothermal ablation : mechanism of tissue injury and current experience in the treatment of tachyarrhythmias. Prog Cardiovasc Dis. 1999;41(6):481-98. [MedLine]
16. Doll N, Kornherr P, Aupperle H, Fabricius AM, Kiaii B, Ullmann C Epicardial treatment of atrial fibrillation using cryoablation in an acute off-pump sheep model. Thorac Cardiovasc Surg. 2003;51(5):267-73. [MedLine]
17. Viola N, Williams MR, Oz MC, Ad N The technology in use for the surgical ablation of atrial fibrillation. Semin Thorac Cardiovasc Surg. 2002;14(3):198-205. [MedLine]
18. Demazumder D, Mirotznik MS, Schwartzman D Biophysics of radiofrequency ablation using an irrigated electrode. J Interv Card Eletrophysiol. 2001;5(4):377-89.
19. Ruchat P, Schlaepfer J, Delabays A, Hurni M, Milne J, Von Segesser LK Left atrial radiofrequency compartmentalization for chronic atrial fibrillation during heart surgery. Thorac Cardiovasc Surg. 2002;50(3):155-9. [MedLine]
20. Santiago T, Melo JQ, Gouveia RH, Martins AP Intra-atrial temperatures in radiofrequency endocardial ablation : histologic evaluation of lesions. Ann Thorac Surg. 2003;75(5):1495-501. [MedLine]
21. Gaynor SL, Diodato MD, Prasad SM, Ishii Y, Schuessler RB, Bailey MS A prospective, single-center clinical trial of a modified Cox maze procedure with bipolar radiofrequency ablation. J Thorac Cardiovasc Surg. 2004;128(4):535-42. [MedLine]
22. Laczkovics A, Khargi K, Deneke T Esophageal perforation during left atrial radiofrequency ablation. J Thorac Cardiovasc Surg. 2003;126(6):2119-20.
23. Breda JR, Breda ASCR, Meneghini A, Freitas ACO, Pires AC Ablação operatória da fibrilação atrial por radiofrequência. Rev Bras Cir Cardiovasc. 2008;23(1):118-22. [MedLine]
24. Wang J, Meng X, Li H, Cui Y, Han J, Xu C Prospective randomized comparison of left atrial and biatrial radiofrequency ablation in the treatment of atrial fibrillation. Eur J Cardiovasc Surg. 2009;35(1):116-22.
25. Beukema WP, Sie HT, Misier AR, Delnoy PP, Wellens HJ, Elvan A Intermediate to long-term results of radiofrequency modified Maze procedure as an adjunct to open-heart surgery. Ann Thorac Surg. 2008;86(5):1409-14. [MedLine]
26. Williams MR, Knaut M, Bérubé D, Oz MC Application of microwave energy in cardiac tissue ablation : from in vitro analyses to clinical use. Ann Thorac Surg. 2002;74(5):1500-5. [MedLine]
27. Gaynor SL, Byrd GD, Diodato MD, Ishii Y, Lee AM, Prasad SM Dose response curves for microwave ablation in the cardioplegiaarrested porcine heart. Heart Surg Forum. 2005;8(5):E331-6. [MedLine]
28. Manasse E, Colombo PG, Barbone A, Braidotti P, Bulfamante G, Roincalli M Clinical histopathology and ultrastructural analysis of myocardium following microwave energy ablation. Eur J Cardiothorac Surg. 2003;23(4):573-7. [MedLine]
29. Manasse E, Medici D, Ghiselli S, Ornaghi D, Galloti R Left main coronary artery lesion after microwave epicardial ablation. Ann Thorac Surg. 2003;76(1):276-7. [MedLine]
30. Williams MR, Argenziano M, Oz MC Microwave ablation for surgical treatment of atrial fibrillation. Semin Thorac Cardiovasc Surg. 2002;14(3):232-7. [MedLine]
31. Vicol C, Kellerer D, Petrakopoulou P, Kaczmarek I, Lamm P, Reichart B Long-term results after ablation for long-standing atrial fibrillation concomitant to surgery for organic heart disease : is microwave energy reliable?. J Thorac Cardiovasc Surg. 2008;136(5):1156-9. [MedLine]
32. Reddy VY, Houghtaling C, Fallon J, Fischer G, Farr N, Clarke J Use of a diode laser balloon ablation catheter to generate circumferential pulmonary venous lesions in an openthoracotomy caprine model. Pacing Clin Electrophysiol. 2004;27(1):52-7. [MedLine]
33. Williams MR, Garrido M, Oz MC, Argenziano M Alternative energy sources for surgical atrial ablation. J Card Surg. 2004;19(3):201-6. [MedLine]
34. Williams MR, Casher JM, Russo MJ, Hong KN, Argenziano M, Oz MC Laser energy source in surgical atrial fibrillation ablation : preclinical experience. Ann Thorac Surg. 2006;82(6):2260-4. [MedLine]
35. Ninet J, Roques X, Seitelberger R, Deville C, Pomar JL, Robin J Surgical ablation of atrial fibrillation with offpump, epicardial, high-intensity focused ultrasound : results of a multicenter trial. J Thorac Cardiovasc Surg. 2005;130(3):803-9. [MedLine]
36. Klinkenberg TJ, Ahmed S, Ten Hagen A, Wiesfeld AC, Tan ES, Zijlstra F Feasibility and outcome of epicardial pulmonary vein isolation for lone atrial fibrillation using minimal invasive surgery and high intensity focused ultrasound. Europace. 2009;11(12):1624-31. [MedLine]
37. Lins RMM, Lima RC, Silva FPV, Menezes AM, Salerno PR, Thé EC, Sepúlveda D, Albuquerque E Tratamento da fibrilação atrial com ablação por ultrassom, durante correção cirúrgica de doença valvar cardíaca. Rev Bras Cir Cardiovasc. 2010;25(3):326-32. [MedLine] View article
38. Brick AV, Seixas TN, Portilho CF, Peres AK, Vieira Jr JJ, Melo Neto R Tratamento intra-operatório da fibrilação atrial crônica com ultra-som. Rev Bras Cir Cardiovasc. 2001;16(4):337-49. View article
39. Groh MA, Binns OA, Burton 3rd HG, Champsaur GL, Ely SW, Johnson AM Epicardial ultrasonic ablation of atrial fibrillation during concomitant cardiac surgery is a valid option in patients with ischemic heart disease. Circulation. 2008;118(14):S78-82. [MedLine]
40. Haïssaguerre M, Jaïs P, Shah DC, Takahashi A, Hocini M, Quiniou G Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med. 1998;339(10):659-66. [MedLine]
41. Wolf RK, Schneeberger EW, Osterday R, Miller D, Merrill W, Flege Jr JB Video-assisted bilateral pulmonary vein isolation and left atrial appendage exclusion for atrial fibrillation. J Thorac Cardiovasc Surg. 2005;130(3):797-802. [MedLine]
42. Gammie JS, Didolkar P, Krowsoski LS, Santos MJ, Toran AJ, Young CA Intermediate-term outcomes of surgical atrial fibrillation correction with the CryoMaze procedure. Ann Thorac Surg. 2009;87(5):1452-8.
43. Cox JL The longstanding, persistent confusion surrounding surgery for atrial fibrillation. J Thorac Cardiovasc Surg. 2010;139(6):1374-86. [MedLine]
44. Barnett SD, Ad N Surgical ablation as treatment for the elimination of atrial fibrillation : a meta-analysis. J Thorac Cardiovasc Surg. 2006;131(5):1029-35. [MedLine]
45. Wolf RK The Wolf Mini-Maze : the official site2010;:2004-09.
46. Kiser AC, Wimmer-Greinecker G, Chitwood WR Totally extracardiac Maze procedure performed on the beating heart. Ann Thorac Surg. 2007;84(5):1783-5. [MedLine]
47. Edgerton JR, Jackman WM, Mack MJ A new epicardial lesion set for minimal access left atrial maze : the Dallas lesion set. Ann Thorac Surg. 2009;88(5):1655-7. [MedLine]
48. Cox JL, Schuessler RB, Lappas DG, Boineau JP An 8 1/2year clinical experience with surgery for atrial fibrillation. Ann Surg. 1996;224(3):267-73.
49. Cappato R, Calkins H, Chen SA, Davies W, Iesaka Y, Kalman J Updated worldwide survey on the methods, efficacy, and safety of catheter ablation for human atrial fibrillation. Circ Arrhythm Electrophysiol. 2010;3(1):32-8. [MedLine]
Article receive on Friday, November 26, 2010
 All scientific articles published at bjcvs.org are licensed under a Creative Commons license
All scientific articles published at bjcvs.org are licensed under a Creative Commons license













All rights reserved 2017 / © 2024 Brazilian Society of Cardiovascular Surgery
DEVELOPMENT BY ![]()
 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}