A 6-year-old female child sought medical service due to a gastrointestinal malformation. During a medical follow-up a partial absence of the inferior vena cava was diagnosed, which is a rare congenital alteration, involving the vascular drainage from the inferior segment of the body. Imaging exams were performed, which contributed to evaluation and description of the case. Conservative treatment with an oral anticoagulant was maintained. The patient presents good evolution after a long-term cardiovascular follow-up.
Criança de 6 anos de idade, sexo feminino, procurou serviço médico devido a mal-formação gastrointestinal. Durante o acompanhamento médico, foi diagnosticada ausência parcial de veia cava inferior, alteração congênita rara que envolve a drenagem vascular do segmento inferior do corpo. Realizados exames de imagem, os quais contribuíram para avaliação e descrição do caso. Mantido tratamento conservador com anticoagulante oral. Paciente apresenta boa evolução após longo tempo de acompanhamento cardiovascular.
INTRODUCTION
The absence of congenital inferior vena cava (IVC) is a rare cardiovascular malformation. It results from atresia of the retrohepatic segment of the IVC during embryogenesis. Most of the time, it is associated with abdominal and cardiac anomalies. Patients without other associated malformations can be asymptomatic and diagnosed serendipitously or as incidental finding on routine imaging examination.
The present study reports a case of inferior vena cava agenesis in a cardiologically asymptomatic patient who sought medical attention due to the presence of gastrointestinal malformation.
CASE REPORT
A 6-year-old female patient in a follow-up program at Hospital de Clínicas da Faculdade de Medicina, Botucatu, São Paulo State, Brazil, due to the presence of imperforate anus (anal atresia), with the rectum opening into the vagina just above the vulva. She underwent surgical procedure in 1997. In 2003, a systolic murmur (+/4) was detected in the precordium. The patient was referred to cardiologic consultation. On physical examination, the child showed the following: heart rate of 92 beats per minute; systemic blood pressure of 110/70 mm Hg; no signs of heart failure. The echocardiogram showed situs solitus in levocardia; basal vessels with normal arrangement; intact interatrial and interventricular septa; normal valves; preserved left ventricle systolic and diastolic function; and undefined cardiovascular anomaly.
For a better evaluation an angiography was performed, which highlighted the partial absence of inferior vena cava with azygos continuation to the left; the blood from the renal infrarenal portions flowing through a large-bore collateral vessel into the hemi-azygos vein that, in its turn, empties in the persistent left superior vena cava, draining into the right atrium through the coronary sinus (Figure 1).
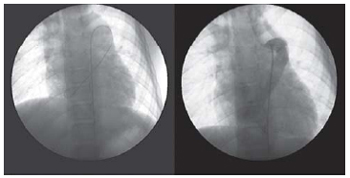
Fig. 1 - Venous angiography shows the catheter-guide and its course throughout hemi-azygos vein and persistent superior vena cava which drains into the right atrium though the coronary sinus
Abdomen and chest CT scans also revealed partial agenesis of the inferior vena cava at suprarenal portion, as well as dilated azygos and hemi-azygos veins (Figure 2). The patient remains under medical follow-up, presenting a 10-year follow-up. Currently, she is cardiologically oligosymptomatic.
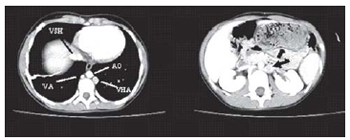
Fig. 2 - Enlarged azygos vein (AV) and hemi-azygos vein (HAV); suprahepatic veins (SHV) and aorta (AO); enlarged azygos system (arrow) to the left of the aorta emptying into the renal veins
The IVC is formed by a complex embryological process between the 6th and 8th weeks of gestation, which coincides with the development of spleen, liver, heart, and lung [1, 2]. This process involves three pairs of primitive veins (posterior cardinal, subcardinal, and supracradinal veins) developing extensive anastomoses among themselves and later on undergo regression and atrophy. The IVC is converted to a unilateral, right-sided consisting, from cauda to cranium, of its postrenal, renal, prerenal, and hepatic segments. When improper completion of the process occurs, several types of IVC anomalies may result, such as IVC partial or total agenesis [3]. In such cases the azygos vein undergo compensatory enlargement to help the venous drainage of the inferior segment of the body.
Approximately 90% of the cases of partial absence of IVC occurs in its suprahepatic segment and may be present in 0.6% to 2% of patients in association to other congenital heart diseases and in 0.3% to 0.5% in other noncardiac anomalies. The most common cardiac defects include dextrocardia, interatrial and interventricular communication, pulmonary stenosis or any combination of these malformations. It may occur in association with transposed abdominal viscera, dygenesis of lung, and polysplenia [4]. These anomalies were not found in our patient. However, the reported case presents with another intestinal congenital malformation (imperforate anus), an association yet not observed and described in English literature.
Regarding the vascular anomaly, the most important subsidies to diagnosis and understanding of this disease were obtained by venous angiography and thoracicoabdominal CT scan. The exams revealed the partial absence of IVC with left-sided azygos continuation; the blood of the renal and infrarenal segments flowing through a enlarged collateral vein into the hemi-azygos vein that, in it is turn, empties into the persistent left superior vena cava; the later drains into the raight atrium through the coronary sinus.
In adults, the IVC congenital changes are reported as accidental during Radiologic work-up or laparotomy. The left-sided enlarged azygos vein can disguise an aortic dissection, a mediastinal mass, or paratracheal adenopathy on the chest radiograph.
Patients without any other associated malformations can remain asymptomatic because the deep venous collateral system involved is sufficiently developed to drain the blood from the lower half of the body into the heart. The patients also present with a cardiac murmur, which can be mistaken with patent ductus arteriosus due to its anatomical topography.
The management of partial absence of IVC is conservative. The importance of knowing this disease is, mainly, to avoid unnecessary surgical interventions. There are reports of even inadvertent ligatures of venous collaterals leading to the death of the patient [1, 6]. However, theoretically, this anomaly may predispose to deep venous thrombosis because an inadequate blood return through the collaterals may increase the venous blood pressure in the veins of lower limb, thereby favoring the venous stasis. Some authors preconize the anticoagulant therapy in these patients [3, 5]. Our patient is on oral anticoagulant therapy, under a 10-year medical follow-up, and remains asymptomatic from the cardiovascular point of view.
CONCLUSION
The absence of IVC can be associated with congenital cardiac and noncardiac anomalies. The present case reports a partial absence of IVC in a patient with imperforate anus. This association has not yet been reported. It is important to be aware of this entity because the literature reports inadvertent ligatures of azygos vein, what is lethal for these patients. Besides, many times we can avoid unnecessary laparotomies and thoracotomies.
REFERENCES
1. Sandercoe GD, Brooke-Cowden GL. Developmental anomaly of the inferior vena cava. ANZ J Surg. 2003;73(5):356-60. [
MedLine]
2. Giordano JM, Trout HH 3rd. Anomalies of the inferior vena cava. J Vasc Surg. 1986;3(6):924-8. [
MedLine]
3. Cho BC, Choi HJ, Kang SM, Chang J, Lee SM, Yang DG, et al. Congenital absence of inferior vena cava as a rare cause of pulmonary thromboembolism. Yonsei Med J. 2004;45(5):947-51. [
MedLine]
4. Yun SS, Kim JI, Kim KH, Sung GY, Lee DS, Kim JS, et al. Deep venous thrombosis caused by congenital absence of inferior vena cava, combined with hiperhomocysteinemia. Ann Vasc Surg. 2004;18(1):124-9. [
MedLine]
5. Hamoud S, Nitecky S, Engel A, Goldsher D, Hayek T. Hipoplasia of the inferior vena cava with azygous continuation presenting as a recurrent leg deep vein thombosis. Am J Med Sci. 2000;319(6):414-6. [
MedLine]
6. Effler DB, Greer AE, Sifers EC. Anomaly of the vena cava inferior; report of fatality after ligation. J Am Med Assoc. 1951;146(14):1321-2. [
MedLine]
 All scientific articles published at bjcvs.org are licensed under a Creative Commons license
All scientific articles published at bjcvs.org are licensed under a Creative Commons license













 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket